

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The unique symptom of intracranial hypotension (IH) is an orthostatic headache caused by low cerebrospinal fluid (CSF) pressure and is not so rare. IH results from loss of CSF caused by a dural defect in the spine, cranial vault, or skull base. The classic orthostatic headache commences within 15 minutes, but occasionally symptoms last up to several hours, after standing or upright sitting position. The criteria of the International Classification of Headache Disorders3) are widely used to diagnose this type of headache. These criteria require at least one of the following to confirm the diagnosis of IH; low CSF pressure; diffuse pachymeningeal enhancement of brain MR imaging; or evidence of CSF leakage on conventional myelography, CT myelography, or radionuclide cisternography (RNC). However, low CSF pressure is not always present in IH.10) A broad spectrum of neuroimaging features has also been recognized in patients with IH,7) particularly diffuse dural enhancement and sagging of the brain on MR imaging.10) However, such diagnostic abnormalities are not always detected.15) RNC and CT myelography are the spinal imaging studies which have been used for identification of the actual site of a CSF leakage. However, in general, neurologists or neurosurgeons do not routinely perform these studies because these invasive modalities required a dural puncture, so that it may worsen the patient's condition; also there are some debates regarding appropriate timing of study.1) At our institution, RNC is routinely performed for patients suspected of having IH.
In this case series, we report two patients in whom IH was suspected. One case showed a false localizing CSF leakage, while the other case showed progressive subdural hematoma (SDH) after epidural blood patch (EBP). The purpose of this case series is to describe the clinical and imaging features of patients with IH.
Case Report
Case 1
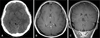
A 56-year-old man was admitted to the emergency department of our hospital due to neck pain and multiple contusions after pedestrian traffic accident. Initial brain computed tomography (CT) scan was grossly normal. Two days later, he complained severe headache. Headache was aggravated by sitting or standing and relieved by lying on his bed. The headache was also accompanied by photophobia, nausea, tinnitus, posterior neck stiffness and progressive somnolence. Follow up brain CT scan showed widening of bilateral frontal and temporal subdural space (Figure 1A). Gadolinium-enhanced brain magnetic resonance imaging (MRI) showed bilateral frontal and temporal subdural space widening and diffuse pachymeningeal enhancement, suggesting IH (Figure 1B, C, D). A subsequent RNC was performed, which revealed mild reflux of radiotracer into the lateral ventricle (Figure 2A). Normal opening pressure and xanthochromia were noted during lumbar puncture. But the supine spinal images demonstrated no evidence of a CSF leakage (Figure 2B). The radiotracer accumulation activity at the left cerebellopontine angle (CPA) cistern was seen, but it was decreased on the 24-hour delayed images (Figure 2A, C). And the both CPA cistern were shown asymmetry on the MRI (Figure 2D). These findings were a false localizing CSF leak at the left ear. In light of the negative investigations, he was managed conservatively with bed rest, hydration, and medication. Two weeks later, he was discharged with no symptoms.
Case 2
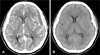
A 31-year-old woman was admitted to the neurosurgical department of our hospital due to severe headache [Visual Analogue Scale (VAS) was 7/10] and vomiting. Initial brain CT showed acute SDH on left cerebral hemisphere (Figure 3A). She had past medical history of operation for hemorrhoid under the spinal anesthesia 2 days ago. Headache was not improved by lying down. Gadolinium-enhanced brain MRI showed acute SDH on left cerebral hemisphere with midline shifting to right and diffuse pachymeningeal enhancement (Figure 3B, C). Lumbar puncture for RNC performed with a 24-gauge needle at the level of L3-L4, revealed an opening pressure of 11 mmH2O and xanthochromia. RNC showed multiple CSF leakage at right anterolateral aspect and left posterolateral aspect of lower lumbar level (Figure 4A, B, C). IH was strongly suspected, and it seemed to be caused by previous spinal anesthesia. Two days after admission, 6 mL of autologous EBP was injected under fluoroscopic guidance between L4 and L5. The patient immediately experienced relief of pain. 8 hours after the EBP, her headache was improved about 5/10 on the VAS. The following day, although the postural headache was not shown, the headache persisted (VAS 4/10). A CT scan performed 2 weeks after EBP showed slightly increased volume of SDH (12 mm at maximal thickness) with aggravation of midline shifting to the right (Figure 5A). Her headache was aggravated (VAS 7/10). We performed burr hole trephination with closed drainage (Figure 5B) and her headache was immediately improved. She was discharge with no focal neurological deficits.
Discussion
IH is an uncommon clinical entity characterized by CSF hypovolemia due to CSF leakage and confirmed with CSF opening pressure of less than 6 cm H2O. Patients with IH often present with postural headache. Other symptoms are often accompanied by postural headache including posterior neck pain or stiffness, and nausea and vomiting and attributable to meningeal irritation which its incidence is approximately 50% of patients.12) Sometimes, it also accompanied by photophobia and less commonly hypacusia and tinnitus, due to vestibulocochlear nerve traction associated with the sagging brain, or transmission of low CSF pressure to the perilymph. Secondary subdural effusions or hematomas may also be the complication of IH, which causes constant, nonpostural headaches. Causes of secondary IH include lumbar puncture, cranial or spinal surgery, and head or spine trauma.11) Incidence of post-lumbar puncture headache is reported at 10% to 30%. In addition to meningeal diverticula, direct mechanical perforation of the dura secondary to degenerative disc-osteophyte is recognized.16)
The diagnosis of IH is difficult, thus careful history taking of patients who suffer from persistent postural headache and selection of proper diagnostic modalities are important. In 18 patients studied by Schievink,12) 17 (94%) received an initial incorrect diagnosis and the median diagnostic delay was 5 weeks. Even some patients had undergone unnecessary invasive procedures including meningeal biopsy, a decompressive craniotomy and the evacuation of subdural fluid collections.
With loss of CSF from the subarachnoid space, total intracranial blood volume is increased to counteract loss of CSF volume. This increases the results in engorgement of the epidural vertebral venous plexus, often most notable in the upper cervical spine; and enlargement and engorgement of the pituitary gland. Gadolinium-enhanced brain MRI is a useful tool for the confirmation of IH. Due to the wide variety of headache patterns, it is better to perform MRI in all patients with unexplained headaches in order to evaluate the possibility of spontaneous intracranial hypotension. However, up to 20% of patients with IH showed neither enhancement nor any other abnormalities on MRI.13) Watanabe et al.15) reported overall the sensitivity for IH was 83% for brain MR imaging and 94% for spinal MR imaging. But high concentration of gadolinium in the subarachnoid space may cause seizures.5) Although MRI has become a first-line diagnostic measure, RNC and CT myelography are particularly useful in identifying CSF leaks and studying CSF circulation.8,17,18) The sensitivity of RNC is lower in case of small leakage. Even when direct findings of tracer extravasation are not visualized, Morioka et al.9) reported that indirect findings on RNC, renal and bladder activity, poor propagation of radiotracer to the convexities, can be useful in determining the presence of leak as well as follow-up monitoring after treatment.
In the first case, the radiotracer accumulation activity at the left CPA cistern was seen; this finding should not be mistaken for identification of actual site of CSF leakage (Figure 2A) because of decreased radiotracer accumulation activity was seen on the 24-hour delayed images (Figure 2C). Furthermore, the both CPA cistern were shown asymmetry on the MRI (Figure 2D). These findings were false localizing finding of CSF leakage at the left ear. Yoon et al.18) reported 15 of 24 cases could not reveal the leakage site. Most patients treated by EBP and showed remarkable improvement. Occasionally CSF pressure within the normal range has been documented in some patients with IH. Orthostatic headache can occur without evidence of IH or detectable CSF leak despite extensive diagnostic testing.
Some cases of IH were resolved spontaneously; thus conservative treatment consisting of bed rest, oral caffeine, and hydration may make sense initially to treat the symptoms during waiting for spontaneous closure of the leakage site. One study showing relief of headache in 75% of patients compared with a control group treated with intravenous saline.14) Once the diagnosis of IH is made, EBP is recommended if conservative treatments fail to reduce symptoms.
The appropriate injection site of EBP is controversial. Some authors reported that the location of EBP is not important, but others suggested that accurate injection on the leakage site is more effective.1,4) Progressive SDH after EBP for IH is extremely rare, there are only three reported cases (Figure 5A, B).2,6,14) Interestingly, all three cases (including our patient) complained of a persistent nonpostural headache after disappearance of the postural headache. This change of symptom suggests that persistent nonpostural headache after EBP might be predictive clue of progressive SDH and that an early CT scan should be performed.
Conclusion
Although the incidence of IH is not so high, it is an important clinical entity to which the clinicians should pay attention. Delayed diagnosis of IH may cause prolongation of symptomatic period and exposes patients to unnecessary, high-risk diagnostic and therapeutic procedures. This report emphasizes that secondary IH can present with various clinical presentations and neuroimaging findings. It also points that the clinicians is to be attentive to alterations of patients' symptoms, in order to prompt management of secondary events during the treatment of IH, such as progression of SDH.



 XML Download
XML Download