

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Ji Woong Oh, MD, Kum Whang, MD, Jhin Soo Pyen, MD, Hyun Ho Jung, MD
Abstract
Objective
The purpose of this study is to evaluate the effect of early mobilization for the patients of chronic subdural hematoma after closed drainage.
Methods
From May 2007 to March 2010, 58 patients with the chronic subdural hematoma treated by closed drainage surgery were included for this study. They were divided into early (EM) and delayed mobilization (DeM) group. We defined the EM group as not only an upright position but also ambulation at the day of operation. And then we evaluated the reoperation rates, duration of hospitalization, cost, postoperative subdural space and complications in each groups.
Results
Among 58 patients, 15 were EM and the others, 43, were DeM. Duration of hospitalization for EM was shorter than that for DeM about 12days (p=0.006). Reoperation rates in EM was 13% and that for DeM was 22%, but it did not show significant difference (p=0.336). Medical cost of DeM was higher than EM. Postoperative subdural space of EM was 10.03 mm, and that of DeM 10.24 mm, which did not showed any significance. And complications, such as pneumonia, ulcer, deep vein thrombosis, were developed in DeM.
Conclusion
EM after closed drainage for chronic subdural hematoma patients showed shorter duration of hospitalization than DeM, also lower cost and fewer complications. And there were no difference between two groups in reoperation rates. EM was better postoperative management methods than DeM after closed drainage.
Figures and Tables
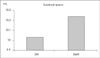
 | FIGURE 1Duration of hospitalization of EM and DeM. Duration of hospitalization for EM was shorter than that for DeM (p=0.0006). EM: early mobilization group, DeM: delayed mobilization group.
|
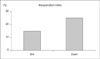 | FIGURE 2Reoperation rates of EM and DeM. Reoperation rates of DeM were higher than EM. But it was not statistically significant (p=0.336). EM: early mobilization group, DeM: delayed mobilization group.
|
 | FIGURE 3Postoperative subdural space in EM and DeM. In DeM group, there were slightly more increased subdural space, but not statistically significant (p=0.8542). EM: early mobilization group, DeM: delayed mobilization group.
|
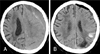 | FIGURE 4This brain computer tomography (CT) was from 75 year-old male patient with chronic renal failure. A: Preoperative CT showed chronic subdural hematoma on left hemisphere. B: Postoperative CT scan on 2nd day, chronic subdural hematoma was almost drained out, but intracerebral hemorrhage was newly developed.
|


References
1. Abouzari M, Rashidi A, Rezaii J, Esfandiari K, Asadollahi M, Aleali H, et al. The role of postoperative patient posture in the recurrence of traumatic chronic subdural hematoma after burr-hole surgery. Neurosurgery. 2007; 61:794–797. discussion 797.

2. Benzel EC, Bridges RM Jr, Hadden TA, Orrison WW. The single burr hole technique for the evacuation of non-acute subdural hematomas. J Trauma. 1994; 36:190–194.
3. Decaux O, Cador B, Dufour T, Jégo P, Cazalets C, Laurat E. [Nonsurgical treatment of chronic subdural hematoma with steroids: two case reports.]. Rev Med Interne. 2002; 23:788–791.
4. F Porchetl NB, Boulard G, Arche DP, Ravussins P. Effet de la position sur la pression intracrhienne. Ann Fr Anesfh RPmim. 1998; 17:149–156.
5. Ito H, Yamamoto S, Komai T, Mizukoshi H. Role of local hyperfibrinolysis in the etiology of chronic subdural hematoma. J Neurosurg. 1976; 45:26–31.
6. Krupa M. [Chronic subdural hematoma a review of the literature. Part 1.]. Ann Acad Med Stetin. 2009; 55:47–52.
7. Kurabe S, Ozawa T, Watanabe T, Aiba T. Efficacy and safety of postoperative early mobilization for chronic subdural hematoma in elderly patients. Acta Neurochir (Wien). 2010.
8. Markwalder TM. Chronic subdural hematomas: a review. J Neurosurg. 1981; 54:637–645.
9. Miele VJ, Sadrolhefazi A, Bailes JE. Influence of head position on the effectiveness of twist drill craniostomy for chronic subdural hematoma. Surg Neurol. 2005; 63:420–423. discussion 423.
10. Miele VJ, Sadrolhefazi A, Bailes JE. Influence of head position on the effectiveness of twist drill craniostomy for chronic subdural hematoma. Surg Neurol. 2005; 63:420–423. discussion 423.
11. Munro D, Merritt HH. Surgical pathology of subdural hematoma based on a stuey of one hundred and five cases. Arch Neurol Psychiatry. 1936; 35:64–78.
12. Murata K. Chronic subdural hematoma may be preceded by persistent traumatic subdural effusion. Neurol Med Chir (Tokyo). 1993; 33:691–696.
13. Nakaguchi H, Tanishima T, Yoshimasu N. Factors in the natural history of chronic subdural hematomas that influence their postoperative recurrence. J Neurosurg. 2001; 95:256–262.
14. Oku Y, Takimoto N, Yamamoto K, Onishi T. Trial of a new operative method for recurrent chronic subdural hematoma. J Neurosurg. 1984; 61:269–272.
15. Lee SC, Kang JK, Jung HT, Dho JO. Factors affecting brain reexpansion after simple burr hole drainage in chronic subdural hematoma. J Korean Neurosurg Soc. 1998; 27:757–762.
16. Suzuki J, Takaku A. Nonsurgical treatment of chronic subdural hematoma. J Neurosurg. 1970; 33:548–553.
17. Grover VK, Bala I, Bandi SS, Mahajan R, Khosla VK. Changes in intracranial pressure in various positions of the head in anaesthetised patients. Bahrain Med Bull. 2003; 25:1–7.
18. Weigel R, Schmiedek P, Krauss JK. Outcome of contemporary surgery for chronic subdural haematoma: evidence based review. J Neurol Neurosurg Psychiatry. 2003; 74:937–943.
 XML Download
XML Download