

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Most of cerebrospinal fluid (CSF) leakages after head trauma are presented within several days and improved by conservative management, although it often needs special procedure, such as lumbar drainage. However, sometimes surgeries are required if patients do not improve by non-surgical treatments. We have experienced one case of 20 year-old man undertaken two operations because of head trauma and nasal CSF leakage, which was presented 29 days after trauma and had not been cured by conservative management. In the operating field, we found the fistula from anterior fossa to nasal cavity. In order to seal the fistula, we used galea flap. We report this case with literature reviews.
Figures and Tables
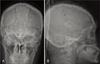
FIGURE 1
PreOP images. AC: Multiple skull fractures, basal skull fractures and facial bone fractures were shown on 3-dimensional computed tomography (CT) reconstruction. D, E: Brain CT demonstrated forehead swelling with pneumocephalus and epidural hematoma on the bifrontal areas. F: 3 hours after trauma hemorrhagic contusion was shown on frontal base.
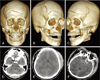
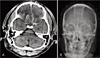
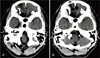
FIGURE 2
PostOP images. A, B: After bilateral decompressive craniectomy, hemorrhagic contusion and swelling of both frontal lobes were shown on the CT.
References
1. Eljamel MS, Foy PM. Post-traumatic CSF fistulae, the case for surgical repair. Br J Neurosurg. 1990; 4:479–483.

2. Friedman JA, Ebersold MJ, Quast LM. Post-traumatic cerebrospinal fluid leakage. World J Surg. 2001; 25:1062–1066.
3. Kim HS, Hur JW, Lee JW, Lee HK. Extraordinarily long-term posttraumatic cerebrospinal fluid fistula. J Korean Neurosurg Soc. 2007; 42:403–405.
4. Martin TJ, Loehrl TA. Endoscopic CSF leak repair. Curr Opin Otolaryngol Head Neck Surg. 2007; 15:35–39.
5. Moza K, McMenomey SO, Delashaw JB Jr. Indications for cerebrospinal fluid drainage and avoidance of complications. Otolaryngol Clin North Am. 2005; 38:577–582.
6. Schick B, Weber R, Kahle G, Draf W, Lackmann GM. Late manifestations of traumatic lesions of the anterior skull base. Skull Base Surg. 1997; 7:77–83.
7. Scholsem M, Scholtes F, Collignon F, Robe P, Dubuisson A, Kaschten B, et al. Surgical management of anterior cranial base fractures with cerebrospinal fluid fistulae: a single-institution experience. Neurosurgery. 2008; 62:463–469. discussion 469-471.
8. Shapiro SA, Scully T. Closed continuous drainage of cerebrospinal fluid via a lumbar subarachnoid catheter for treatment or prevention of cranial/spinal cerebrospinal fluid fistula. Neurosurgery. 1992; 30:241–245.
9. Stewart BT, Kaye AH. Delayed cerebrospinal fluid rhinorrhoea: a case report. Aust N Z J Surg. 1992; 62:818–820.
 XML Download
XML Download