

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Trapped 4th ventricle hydrocephalus (TFVH) is occasionally presented as a series of sequel which came after inflammatory condition of central nervous system (CNS). Treatment of TFVH with intervention may aid preservation of life and neurological function. This is a report of TFVH patient who underwent improvement of neurology without complication, after navigation assisted lateral transcerebellar ventriculo-peritoneal (V-P) shunt system application. A Thirty-four years-old, female came to hospital with gait disturbance and dizziness. She had history of V-P shunt operation at lateral ventricle because of hydrocephalus due to listeria meningitis. General work-up and imaging study performed, and no other specific new finding except enlargement of 4th ventricle. The cause of dizziness and syncope was deduced as TFVH. With Stealth navigation system's assistance, lateral transcerebellar (LTC) V-P shunt had planned. With navigation system's guidance, proximal catheter insertion was performed with confirmation of clear cerebrospinal fluid (CSF) drainage. Then, using 3-way connector, proximal catheters located at lateral and 4th ventricle was connected to form a one way out system. Two proximal catheters and one valve system finally set. Patient's symptoms and hydrocephalus were gradually improved with shunt pressure management without specific complications. Complication of brainstem penetration with LTC V-P shunt for the treatment of TFVH may be reduced with navigation assistance technique. So, we are expecting more easy concern of LTC approach for the treatment of TFVH, by this technique.
Figures and Tables
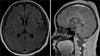 | FIGURE 1Initial magnetic resonance imaging before 1st ventriculoperitoneal shunt operation. There were no specific intracranial findings, except subgaleal hematoma at right parietal area, extracranial. The patient had minimal head trauma history, at about 1 month before imaging study.
|
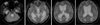 | FIGURE 2Diffusion magnetic resonance image after seizure and mental change. Diffuse enlargements of both lateral ventricle and 3rd ventricle enlargement were identified, which were compatible with acute hydrocephalus.
|
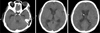 | FIGURE 3Computed tomography scan after 1st external ventricular drainage procedure. Hydrocephalus was improved with procedure.
|
 | FIGURE 4Computed tomography scan after 1st ventriculoperitoneal shunt operation at right lateral ventricle. Hydrocephalus' improvement was maintained after operation.
|
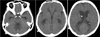
 | FIGURE 5Imaging study at 2nd admission. A: Computed tomography scan. 4th ventricle enlargement was obviously identified. B: Magnetic resonance imaging after modulation of shunt system's valve pressure. The size of both lateral ventricles was improved, but 4th ventricle was still enlarged with T2 FLAIR's high signal change around 4th ventricle. FLAIR: fluid-attenuated inversion recovery.
|


References
1. Alberti O, Dorward NL, Kitchen ND, Thomas DG. Neuronavigation--impact on operating time. Stereotact Funct Neurosurg. 1997; 68:44–48.
2. Asai A, Hoffman HJ, Hendrick EB, Humphreys RP. Dandy-Walker syndrome: experience at the Hospital for Sick Children, Toronto. Pediatr Neurosci. 1989; 15:66–73.

3. Barnett GH, Kormos DW, Steiner CP, Weisenberger J. Use of a frameless, armless stereotactic wand for brain tumor localization with two-dimensional and three-dimensional neuroimaging. Neurosurgery. 1993; 33:674–678.
4. Chai WX. Long-term results of fourth ventriculo-cisternostomy in complex versus simplex atresias of the fourth ventricle outlets. Acta Neurochir (Wien). 1995; 134:27–34.
5. Coker SB, Anderson CL. Occluded fourth ventricle after multiple shunt revisions for hydrocephalus. Pediatrics. 1989; 83:981–985.
6. Colli BO, Pereira CU, Assirati Júnior JA, Machado HR. Isolated fourth ventricle in neurocysticercosis: pathophysiology, diagnosis, and treatment. Surg Neurol. 1993; 39:305–310.
7. Colpan ME, Savas A, Egemen N, Kanpolat Y. Stereotactically-guided fourth ventriculo-peritoneal shunting for the isolated fourth ventricle. Minim Invasive Neurosurg. 2003; 46:57–60.
8. Dandy WE. The diagnosis and treatment of hydrocephalus due to occlusions of the foramina of Magendie and Luschka. Surg Gynecol Obstet. 1921; 32:112–124.
9. Dorward NL, Paleologos TS, Alberti O, Thomas DG. The advantages of frameless stereotactic biopsy over frame-based biopsy. Br J Neurosurg. 2002; 16:110–118.
10. Eller TW, Pasternak JF. Isolated ventricles following intraventricular hemorrhage. J Neurosurg. 1985; 62:357–362.
11. Hall WA. The safety and efficacy of stereotactic biopsy for intracranial lesions. Cancer. 1998; 82:1749–1755.
12. Harrison HR, Reynolds AF. Trapped fourth ventricle in coccidioidal meningitis. Surg Neurol. 1982; 17:197–199.
13. Harter DH. Management strategies for treatment of the trapped fourth ventricle. Childs Nerv Syst. 2004; 20:710–716.
14. Hesselmann V, Wedekind C, Terstegge K, Schulte O, Voges J, Krug B, et al. An isolated fourth ventricle in neurosarcoidosis: MRI findings. Eur Radiol. 2002; 12:Suppl 3. S1–S3.
15. Hubbard JL, Houser OW, Laws ER Jr. Trapped fourth ventricle in an adult: radiographic findings and surgical treatment. Surg Neurol. 1987; 28:301–306.
16. Karachi C, Le Guérinel C, Brugiéres P, Melon E, Decq P. Hydrocephalus due to idiopathic stenosis of the foramina of Magendie and Luschka. Report of three cases. J Neurosurg. 2003; 98:897–902.
17. Lee M, Leahu D, Weiner HL, Abbott R, Wisoff JH, Epstein FJ. Complications of fourth-ventricular shunts. Pediatr Neurosurg. 1995; 22:309–313.
18. Lourie H, Shende MC, Krawchenko J, Stewart DH Jr. Trapped fourth ventricle: a report of two unusual cases. Neurosurgery. 1980; 7:279–282.
19. Mohanty A. Endoscopic third ventriculostomy with cystoventricular stent placement in the management of dandy-walker malformation: technical case report of three patients. Neurosurgery. 2003; 53:1223–1228.
20. Montgomery CT, Winfield JA. Fourth ventricular entrapment caused by rostrocaudal herniation following shunt malfunction. Pediatr Neurosurg. 1993; 19:209–214.
21. Raimondi AJ, Samuelson G, Yarzagaray L, Norton T. Atresia of the foramina of Luschka and Magendie: the Dandy-Walker cyst. J Neurosurg. 1969; 31:202–216.
22. Rakate HL. Hydrocephalus classification and pathophysiology. In : McLone DG, editor. Pediatric neurosurgery: surgery of the developing nervous system. Philadelphia: Saunders;2001. p. 457–474.
23. Sharma RR, Pawar SJ, Devadas RV, Dev EJ. CT stereotaxy guided lateral trans-cerebellar programmable fourth ventriculo-peritoneal shunting for symptomatic trapped fourth ventricle. Clin Neurol Neurosurg. 2001; 103:143–146.
24. Villavicencio AT, Wellons JC 3rd, George TM. Avoiding complicated shunt systems by open fenestration of symptomatic fourth ventricular cysts associated with hydrocephalus. Pediatr Neurosurg. 1998; 29:314–319.
25. Zimmerman RA, Bilaniuk LT, Gallo E. Computed tomography of the trapped fourth ventricle. AJR Am J Roentgenol. 1978; 130:503–506.
 XML Download
XML Download