

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Pneumocephalus is defined as the presence of air or gas within the cranial cavity. It is a relatively common complication of basal skull fractures, brain abscesses, and bone erosion as a result of an intracranial tumor and cerebrospinal fluid (CSF) diversion procedures.2,5,7,11) Although most cases of pneumocephalus resolve spontaneously, pneumocephalus occupying a large space in the intracranial cavity leads to the development of headache, restlessness, confusion, disorientation and neurologic deterioration, which sometimes requires surgical procedures.1,5,7,13,17) A subarachnoidpleural fistula following thoracic spinal fracture associated with a pneumothorax and thoracotomy for a Pancoast tumor may also result in pneumocephalus.6,8,16) However, there are only a few studies documenting pneumocephalus associated with spinal surgery.10,14) We report a case of symptomatic pneumocephalus after surgery for a spinal intradural tumor.
Case Report
A 30-year-old man presented with a 12-month history of increasing low back and bilateral leg pain. On physical examination, there was no significant neurological abnormality detected. A magnetic resonance imaging (MRI) scan of the lumbar spine demonstrated a well-demarcated, intradural extramedullary tumor at the level of L3-4. The lesion appeared hyperintense on a T1-weighted image after intravenous contrast injection (Figure 1). After unilateral laminectomy with bilateral decompression at L3 and 4, we opened the dura; this exposed a pinkish, solid, encapsulated mass that measured 1.0×1.4×1.2 cm, arising from the filum terminale and overlying adherent nerve roots of the cauda. Microscopy revealed that the mass appeared to have no rootlets adherent to its base. We performed an en-bloc total resection. We then flushed the surgical cavity out continuously with normal saline. The dura was closed with tissue adhesives so it would be watertight. Histopathological examination identified the tumor as a myxopapillary ependymoma. It revealed cuboidal to elongated tumor cells radially arranged in a papillary manner and around the vascularized stromal cores in a mucoid background (Figure 2). The patient had no problem postoperatively such as CSF leakage. We encouraged the patient to assume a sitting position after 6 hours.
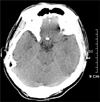
The patient presented with late onset headache after sitting position. Although he was administered analgesics, he became worse with the development of restlessness. A computed tomography (CT) scan showed pneumocephalus bilaterally in the sylvian and basal cisterns (Figure 3). The patient experienced a full recovery with bed rest and hyperhydration.
On the 10th postoperative day, a follow-up CT scan was free of air in the subarachnoid space in the brain (Figure 4). The patient was discharged without any neurological sequelae on the 14th postoperative day.
Discussion
The most frequent cause of pneumocephalus is head trauma followed by intracranial neoplasms, infections, neurosurgery, paranasal surgery, and diagnostic or neurosurgical interventions such as a lumbar puncture.2,4,5,7,11) A skull fracture with a dural tear allows the communication of air into the subarachnoid space, resulting in pneumocephalus. The mechanism responsible for pneumocephalus is explained by the following two factors. First, the ball-valve mechanism explains that air enters the intracranial cavity through a defect whenever the extracranial pressure exceeds the intracranial pressure.13) Second, the inverted bottle mechanism explains that continuous leakage of CSF results in a relatively negative intracranial pressure, thereby allowing replacement of lost fluid by air.11,13) Pathophysiologically, the mechanism of development of pneumocephalus associated with spinal surgery was also based on these factors.10,14) Most surgeons already know about the possibility of developing pneumocephalus after many kinds of surgeries involving opening of the dura. Therefore, surgeons usually pay careful attention to minimize CSF leakage and continue to irrigate saline continuously into the surgical cavity during the surgery. However, a review of the literature revealed that there have been no reports except a few papers10,14) about the development of pneumocephalus after surgery for a spinal intradural tumor. Ozturk et al. reported that a patient who underwent pedicle screw fixation for thoracolumbar scoliosis developed pneumocephalus after the surgery. A pedicle screw coursed through the spinal canal at the L2 level, and it resulted in a dural tear and CSF leakage. Pneumocephalus associated with infratentorial and supratentorial hemorrhage developed due to a negative intracranial pressure.10) Turgut et al.14) reported that a symptomatic tension pneumocephalus developed due to iatrogenic CSF leakage following surgical intervention and drainage with a vacuum suction device for a lumbar disc herniation. A thoracic spine fracture or thoracotomy may result in dural and pleural tears resulting in a subarachnoid-pleural fistula, leading to the development of pneumocephalus associated with a pneumothorax.6,8,16)
Air within the spinal canal is defined as pneumorrhachis.9) The subarachnoid space extends from the basal cisterns surrounding the brainstem superiorly to its termination at the level of the sacral vertebra. In the case of a skull fracture, subarachnoid pneumorrhachis is resulted from pneumocephalus, whereby air from the subarachnoid space of the brain migrates into the spine; this usually occurs when the patient is in the face-down position, letting air migrate through the foramen magnum.3) However, in our case, the contrary occurred. We think that the air might have been entrapped in the surgical cavity when the tumor burden was removed en-bloc. When the patient assumed a head-up position during the postoperative period, the subarachnoid air migrated from the spine into the brain. That is to say, that air floats up the spinal canal into the brain.
Pneumocephalus usually tends to reabsorb with conservative management. It requires bed rest and hyperhydration. However, tension pneumocephalus is symptomatic and associated with severe headache and restlessness or even neurological deterioration. It requires immediate surgical procedures.5,7,13) These include simple aspiration through burr holes,1) use of a closed water-seal drainage system to promptly reduce the intracranial pressure and to maintain the persistent pressure gradient between intracranial and extracranial for closure of the dural fistula,1,7) or reconstruction of the injured sites.17)
It requires attention to prevent pneumocephalus from developing during spinal tumor surgery. Turgut et al. recommends that inhalational nitrous oxide not be used; they also recommend that using 5 cmH20 positive end-expiratory pressure (PEEP) may reduce the occurrence of pneumocephalus by increasing the intrathoracic pressure and minimizing the negative pressure effect that occurs during surgery for a spinal intradural tumor.15) The tumor should be removed meticulously. One then needs to flush out the air in the surgical cavity completely with continuous normal saline to prevent its entering into the surgical cavity, prior to closing the dural mater. Furthermore, there needs to be a watertight dural closure to minimize CSF leakage and maintenance of adequate hydration for proper cerebral perfusion.12)



 XML Download
XML Download