

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Methods
Ethics
Subjects
Sample Size
Study Design
Plasma Aceclofenac Assay
Pharmacokinetics Analysis
Safety Assessment
Statistical Analysis
Results
Study Participants
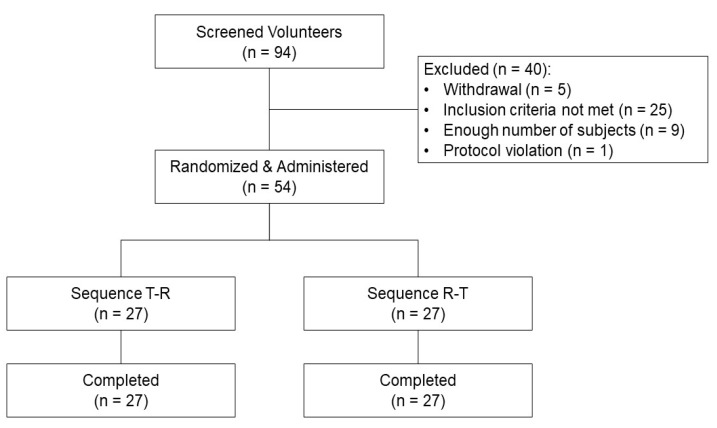 | Figure 1Subject disposition. Abbreviations: Sequence T–R, a fixed-dose combination tablet of SKI306X 300 mg /aceclofeanc 100 mg once (treatment T) was administered first in period 1, then co-administration of 300 mg of SKI306X and 100 mg of aceclofenac as individual tablets once (treatment R) in period 2; Sequence R–T, treatment R first in period 1, then treatment T in period 2.
|
Table 1
Demographics and baseline characteristics of the study population
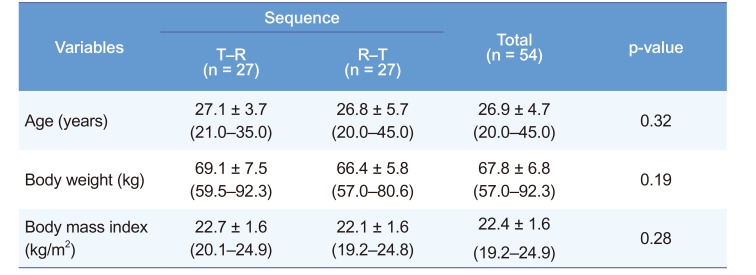
Notes: The data are expressed as the mean ± SD (min–max). Abbreviations: Sequence T–R, a fixed-dose combination tablet of SKI306X 300 mg /aceclofenac 100 mg once (treatment T) was administered first in period 1, then co-administration of 300 mg of SKI306X and 100 mg of aceclofenac as individual tablets once (treatment R) in period 2; Sequence R–T, treatment R first in period 1, then treatment T in period 2. The p-values between the two groups in each part were calculated using the Wilcoxon rank sum test. There were no statistically significant differences in age, body weight, and body mass index.
![]()
Pharmacokinetics Parameters
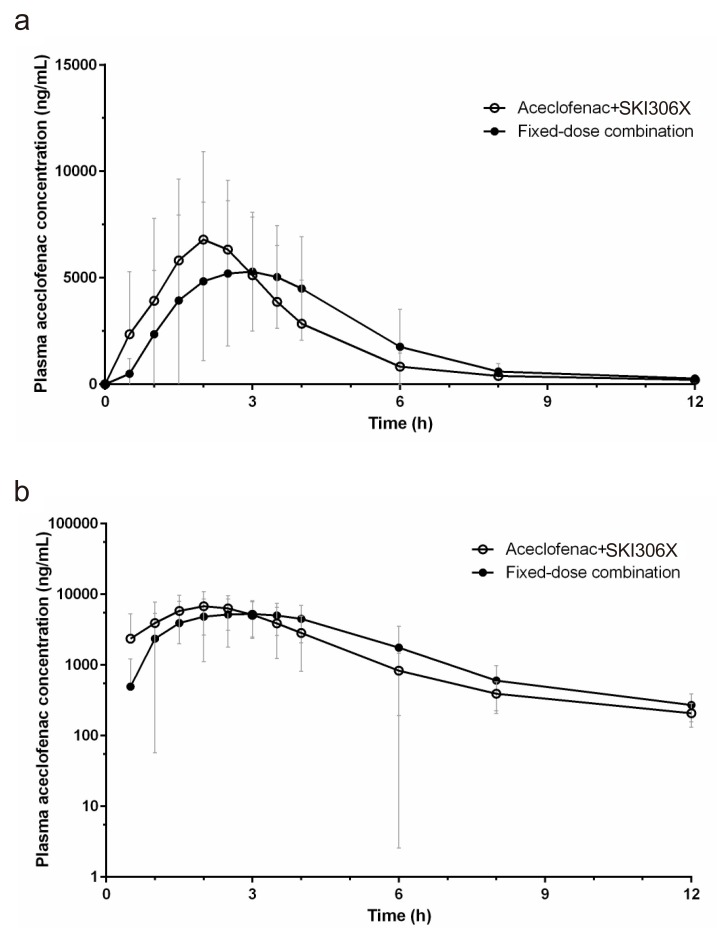 | Figure 2Mean (SD) plasma concentration-time profiles of aceclofenac (a: linear scale, b: semi-logarithmic scale).
|
Table 2
Pharmacokinetic parameters of aceclofenac after the administration of a fixed-dose combination tablet that included 300 mg of SKI306X and 100 mg of aceclofenac once (treatment T) and co-administration of a SKI306X 300 mg and an aceclofenac 100 mg once (treatment R) in healthy volunteers
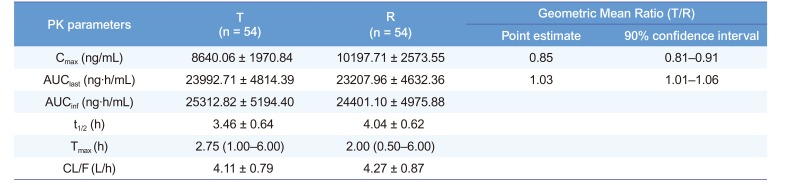
Notes: The values are presented as the mean ± SD, except for the tmax, which is presented as the median (range). Abbreviations: PK, pharmacokinetic; Cmax, maximum plasma concentration of the drug; AUClast, area under the plasma concentration-time curve from the dosing time to the last measurable concentration; AUCinf, AUC from the dosing time extrapolated to infinity; t1/2, elimination half-life; Tmax, time to Cmax; CL/F, apparent total clearance.
![]()
Safety
Table 3
Summary of adverse events
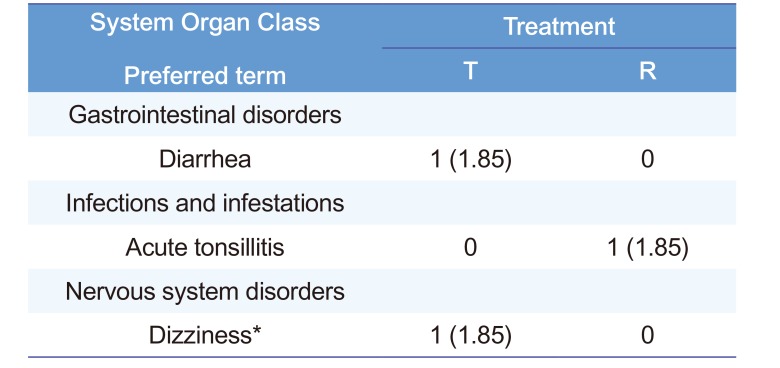
| System Organ Class Preferred term | Treatment | |
|---|---|---|
| T | R | |
| Gastrointestinal disorders | ||
| Diarrhea | 1 (1.85) | 0 |
| Infections and infestations | ||
| Acute tonsillitis | 0 | 1 (1.85) |
| Nervous system disorders | ||
| Dizziness* | 1 (1.85) | 0 |
Notes: The data are expressed as the number (%) of adverse events. *Dizziness is considered as drug-related AE. Abbreviations: T, treatment group administered a fixed-dose combination tablet that included 300 mg of SKI306X and 100 mg of aceclofenac once; R, treatment group administered 300 mg of SKI306X and 100 mg of aceclofenac concomitantly once.
![]()
 XML Download
XML Download