

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The presence of insufficient bone volume leads to the necessity of bone-grafting procedures to reconstruct the alveolar ridge prior to implantation in order to achieve a predictable long-term prognosis [1].
Several grafting techniques using autografts, xenografts, allografts, and alloplastic materials have been implemented in oral surgery for lateral augmentation [23]. Autografts exhibit important biological properties such as osteoconduction, osteoinduction, and osteogenesis to different extents [4], and are still considered to be the gold standard in alveolar ridge augmentation [56]. A major concern in the use of autologous bone grafts is the risk of bone resorption after transplantation [7].
Depending on the size and the morphology of the bony defect, multiple grafting techniques can be distinguished. In addition to the application of block bone grafts, particulated bone augmentation has been used successfully for the reconstruction of alveolar ridge deficiencies, but further research is necessary for a definitive assessment and to determine the efficacy of this approach [89].
Based on their different embryologic origins, membranous and endochondral bone grafts have been thought to exhibit different properties. However, the morphology and the three-dimensional microarchitecture are considered to be more important factors in the survivability of bone transplants [10].
Due to the close proximity of the donor and grafting sites, conventional surgical accessibility, reduced donor site morbidity, the lack of cutaneous scarring, and shorter hospitalisation time, intraoral bone grafting is favoured when only small amounts of bone are needed [511]. Furthermore, harvesting bone from the symphysis/chin and grafting bone from the ramus/retromolar have been described as techniques capable of treating localised defects [51213]. Multiple studies have investigated the morbidity related to different grafting approaches, finding bone transplantation from the ramus area to be advantageous [5131415]. Despite reduced donor site morbidity and overall patient satisfaction related to the surgical approach, bone resorption over time after autologous bone augmentation is a major concern.
In the literature, minimal data have been published regarding the clinical evaluation and resorption tendencies of bone augmentation procedures with autologous bone grafts from the posterior mandible [513]. In fact, no long-term data about bone level changes are yet available. It is known that the evaluation of peri-implant bone conditions is important for assessing the long-term success and survival rates of dental implants in augmented bone.
The aim of the present study was to analyse long-term crestal bone changes and implant survival after particulated autologous bone grafting from the retromolar region.
MATERIALS AND METHODS
Patients
In this retrospective study, 109 patients with alveolar ridge deficiencies of the maxilla and the mandible were involved. All patients were recruited from a private office and had been treated with retromolar bone grafting prior to the insertion of endosseous dental implants.
Surgery and implant procedure
All surgical procedures were performed under local anaesthesia (Ultracain DS forte, articaine with epinephrine 100,000:1; Sanofi, Paris, France) and sterile conditions. Dissection of the local mucoperiostal flaps by a crestal incision and vertical relief cut was performed in order to uncover the augmentation site. The bone graft donor site was uncovered by a horizontal incision in the oral vestibule starting from the first molar and extending to the ascending ramus of the mandible, creating a mucoperiostal flap. Retromolar bone was harvested by a combined approach, comprising a trepan bur (Hu-Friedy, Chicago, IL, USA) and a bone chisel (Aesculap, Braun Melsung AG, Melsung, Germany).
After weakening the bone with the bur, bone blocks were obtained with a chisel. The bone blocks were further processed with a bone mill (R. Quétin Bone-Mill, Dental Products, Leimen, Germany) in order to generate particulated bone chips, which were used for the following augmentation procedure.
The donor site defect was filled with collagenous material (TissueFleece, Baxter International, Deerfield, IL, USA) depending on the size and shape and subsequently closed with non-resorbable mucosal sutures (Ethilon, Ethicon, Somerville, NJ, USA and Terylene, Serag Wiessner, Naila, Germany) after repositioning the mucosal flap.
Depending on the bone quantity and quality, autologous bone grafting was performed with simultaneous or staged implantation (after four to six months). In cases where a large amount of bone was needed in the vertical and horizontal directions, with more than 5 mm at the augmentation site, bone grafting and implantation were carried out in a two-stage procedure. In order to reconstruct the buccal site of the alveolar crest, the bony defect was filled with particulated bone and densified (Hu-Friedy).
The particulated bone used for horizontal bone augmentation was covered with resorbable (Bio Guide, Geistlich Biomaterials, Baden-Baden, Germany), non-resorbable membranes (FRIOS BoneShields, Dentsply International, York, PA, USA), or without any kind of material, depending on the defect size. Bony defects smaller than 5 mm below the implant shoulder were covered with resorbable material. In cases of a bony defect <5 mm and merely a thin layer of mucosal tissue, no material was used. Defects larger than 5 mm, up to a total loss of the buccal site, were covered with non-resorbable materials. Fixation of the non-resorbable material was performed using pins (FRIOS Membrane Tacks, Dentsply International). The non-resorbable material was removed during the implantation procedure or implant exposure procedure.
Approximately four to six months after the augmentation procedure, the implants were inserted according to the manufacturer’s surgical protocol for each of the four different implant systems (Camlog Biotechnologies, Winsheim, Germany; Nobel Biocare, Zuerich, Switzerland; Semados, Bego Bremer Goldschlägerei Wilh. Herbst GmbH & Co. KG, Bremen, Germany; Straumann AG, Basel, Switzerland). The Camlog, Nobel Biocare and Semados implants were inserted epicrestally and the Straumann implants with sandblasted acid etched surface (SLA) were placed along the smooth-rough border. In order to achieve consistency, bone quality was assessed based on its clinical appearance using the D1–D4 Misch scoring system by the same surgeon throughout the study [16]. Implant stability of the dental fixture was measured by assessing insertion torque with a ratchet and categorised as follows: primary stability (torque >30 N∙cm) or no primary stability (torque <30 N∙cm).
All patients were clinically evaluated after two, seven, and 40 days as well as after four to six months. The clinical evaluation included the assessment of complications such as inflammation, mucosal erythema, wound dehiscence, and loss of bone grafts.
Radiological evaluation
Radiographic follow-up was carried out to evaluate dimensional crestal bone changes after the implantation, as well as at one, three, five, seven and 10 years after implantation. The quantitative evaluation of peri-implant bone loss was performed on routinely taken panoramic radiographs (Trophy Orthopantomograph OP 100, Trophy Radiologie GmbH, Kehl, Germany; Gendex Orthoralix 9200 DDE, Gendex, Hatfield, PA, USA; Orthophos XG 3D ready, Sirona Dental Systems, Wals, Austria), as described in a previous study [17]. However, more than 90% of all images were taken using the Gendex Orthoralix 9200 DDE.
The bone measurements of the marginal vertical changes were performed with the imaging software of the corresponding X-ray equipment provider (Sidexis, Sirona Dental Systems; Trophy Imaging Software, Trophy Radiologie GmbH; VixWinPlatinum, Gendex) by a single investigator three times at three different time points to perform quantification using the method described by Gomez-Roman et al. [18]. The reference point was the level of the abutment-implant interface. The interpretation of the mean values of the mesial and distal sites were performed separately. The mean crestal bone changes were analysed by subtracting the mean values of bone loss from the initial postoperative value.
Statistics
The collected data were analysed descriptively using SPSS version 23.0 (IBM Corp., Armonk, NY, USA) and SAS version 9.1 (SAS Institute Inc., Cary, NC, USA). Graphical illustrations were created using PRISM 5 (GraphPad Software, Inc., La Jolla, CA, USA).
Implant survival was evaluated using Kaplan-Meier analysis. The correlation between the bone crestal changes and the age were analysed using Spearman's rank-order correlation coefficient. The Mann-Whitney-U-test was used to evaluate differences between the crestal bone level changes and the gender, localisation (mandible vs. maxilla), nicotine abuse, the one-stage/two-stage method, as well as implant stability. The impact of the implant system and the usage of membrane material and type were analysed using the Kruskal-Wallis test. In order to ensure comparability between the imbalance of data (resorbable and non-resorbable membrane, one-stage/two-stage method, the statistical analysis was extended by adding the exact test. The mesial and distal sites were analysed separately. P-values <0.05 were considered to indicate statistical significance.
RESULTS
Patients
A total of 109 patients (68 female, 41 male) received 164 implants from four different manufacturers (Table 1) between September 1999 and April 2005. The patients ranged in age from 23 to 73 years (mean age, 51.09±11.65 years). Chronic nicotine abuse was noted in 113 patients, while 51 patients were non-smokers.

Implants
Overall, 97 implants were placed in the upper jaw and 67 implants were placed in the lower jaw. The anatomical distribution of the dental implant placement is illustrated according to the Fédération Dentaire Internationale in Figure 1.

Resorbable membranes were used in 110 cases and non-resorbable membranes were used in 23 cases to cover the augmentation region. However, 31 cases were treated without the usage of any membrane material. Bone quality differed between patients. Ninety-four implants were inserted in bone with bone quality D3, followed by 62 implants inserted in D2-quality bone, six implants in D4-quality bone, and two implants were implanted in D1-quality bone. Initial implant stability, with a torque >30 N∙cm, was achieved in the insertion of 151 implants, while 13 implants were placed with less than 30 N∙cm of torque stability. Depending on the bone quality and quantity available in the insertion area, autologous bone grafting was carried out with simultaneous (n=154) or staged (n=10) implantation. The mean observation period was 105.26±21.58 months after implantation.
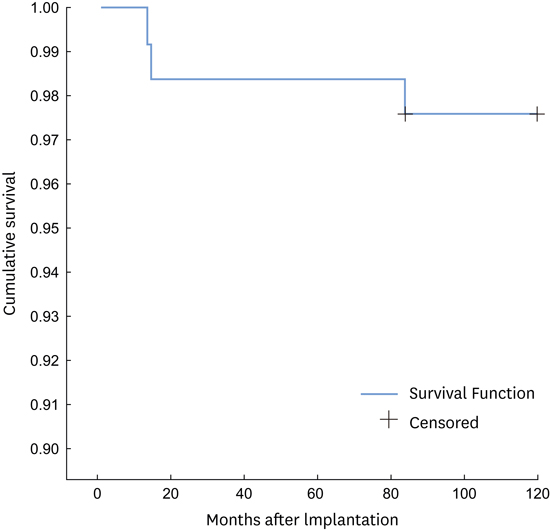
During the observation period, four implants (NobelReplace, n=1; Straumann SLA, n=3) were lost due to a lack of osseointegration, peri-implantitis, or unsuitable loading. Implants were lost at different time points after implantation and were located in the upper (n=2) and lower (n=2) jaw. At one month, an implant was lost in region 34; at 14 months, in region 22; at 15 months, in region 40; and at 84 months, in region 46. The 10-year Kaplan-Meier survival rate was 97.6%. The overall Kaplan-Meier survival rate for the observation period of the implants is presented in Figure 2.
 | Figure 2Cumulative implant survival over time. Kaplan-Meier survival analysis for implants placed in augmented bone. The diagram shows the overall survival of all implants for an observation period of 10 years.
|
The mean values of mesial and distal crestal bone changes over time are presented in Table 2. Due to loss to follow-up, only 103 implants had a follow-up period of 10 years, whereas 146 implants were followed up for five years and 144 implants were followed up for seven years after insertion. The differences in peri-implant bone loss over time are displayed in Figures 3 (mesial) and 4 (distal).
Table 2
Mean values of mesial and distal crestal bone changes over time, with 95% confidence intervals

![]()
 | Figure 3Differences in mesial peri-implant bone loss between follow-up time points.
t1= difference of crestal changes between one year and the postoperative value.
t2= difference of crestal changes between three and one year.
t3= difference of crestal changes between five and three years.
t4= difference of crestal changes between seven and five years.
t5= difference of crestal changes between ten and seven years.
|
 | Figure 4Differences in distal peri-implant bone loss between follow-up time points.
t1= difference of crestal changes between one year and the postoperative value.
t2= difference of crestal changes between three and one year.
t3= difference of crestal changes between five and three years.
t4= difference of crestal changes between seven and five years.
t5= difference of crestal changes between ten and seven years.
|
A significant difference was found in crestal bone loss depending on the implant system (Pmesial/distal<0.001). Straumann implants showed significantly less mean crestal bone loss. Due to the small number of dental implants, the Semados implant (n=1) was not included in the analysis. Statistical analyses showed a highly significant relationship between primary stability and mean crestal bone loss (Pmesial<0.001, Pdistal=0.002).
No significant effect on mean crestal bone loss was observed for age (Pmesial=0.677, Pdistal=0.866), gender (Pmesial=0.149, Pdistal=0.296), localization in the maxilla versus the mandible (Pmesial=0.073, Pdistal=0.057), bone quality (Pmesial=0.161, Pdistal=0.272), time of implant placement (Pmesial=0.252, Pdistal=0.443), use of a membrane (Pmesial=0.726, Pdistal=0.489), or nicotine abuse (Pmesial=0.687, Pdistal=0.598).
DISCUSSION
Autologous bone grafting procedures offer great potential in the reconstruction of alveolar ridge deficiencies caused by a variety of pathological conditions. The purpose of the present study was to evaluate the long-term success of implants and bone level changes after a retromolar augmentation procedure.
One way to evaluate the success of implantation after bone augmentation is to determine the overall long-term implant survival. Depending on the augmentation procedure, donor site, implant type, usage of a membrane barrier and loading regime, survival rates have been reported to range between 60% and 100% [719]. In a prospective study after vertical augmentation with particulate bone, Simion et al. [20] reported an implant survival of 100%, but with a mean follow-up of only 12 months. Another case study documented a success rate of 100% after 36 months [21].
Within the present study, an overall survival rate of 97.6% after 10 years was documented. Moraschini et al. [22] presented comparable results, finding a mean survival rate of 94.6% after a 10-year period of follow-up observation after implantation without prior bone augmentation procedures. Tinsley et al. [23] reported a peak in the implant failure rate between the first and second year after implantation with a subsequent decrease over time. This is in agreement with our results, which indicated that the highest incidence of implant failure occurred one to two years after implantation. However, long-term implant survival after autologous bone transplantation is often related to peri-implant bone loss, which is a major concern in implantology. Sufficient osseointegration of dental implants is a major predictive factor for long-term implant survival [24], as well as peri-implant bone conditions.
In accordance with the present results, based on particulated bone grafts from intraoral donor sites, Verhoeven et al. [25] observed a non-linear resorption process, in which pronounced bone loss took place during the first year after iliac crest onlay bone graft augmentation in atrophic mandibles. Similar findings have been reported after bone augmentation of a mandible with an avascular fibula [26] and iliac bone [27]. Those findings correspond to the results of the present study. The greatest peri-implant bone changes were seen in the first year, followed by a decrease in bone resorption over time. However, no comparable long-term studies investigating the peri-implant resorption rate of retromolar particulated bone grafts are currently available in the literature. Some data exist regarding bone level changes after augmentation with autologous bone blocks from the ramus of the mandible, but the authors only documented a mean follow-up of 12 months [28] or 19 months [29]. Furthermore, details about the insertion depth of the implants are missing [29].
In the present study, the results revealed a relationship between the implant system and bone level changes. Straumann SLA implants presented the least peri-implant bone resorption in comparison with implants from other manufacturers. This may have been related to the tissue-level design. SLA implants are inserted supracrestally, which avoids a micro-gap (implant-abutment interface) between the implant and abutment at the crestal bone level. Studies have indicated that a relationship may exist between peri-implant bone changes and the tissue-level design with respect to the location of the rough-smooth border in relation to the alveolar crest [3031].
Previously, the embryological origin of bone was thought to be crucial for implant survival, but currently the ratio of cortical to cancellous bone seems to be more important [1032]. In addition, Sugg et al. [33] have demonstrated the importance of graft microarchitecture in the context of the local mechanical environment.
Compared to en bloc bone transplants shaped with cortical or cancellous bone, particulated bone does not exhibit structural integrity. This construct features a honeycomb-like structure that allows the unobstructed ingrowth of vascular tissue. A study with small and large allogeneic particulated bone particles demonstrated that in addition to localization, the size of bone chips influenced the resorption and replacement rate [34]. To date, no study has evaluated these parameters with autologous bone.
Primary stability is considered a major factor influencing implant success [3536]. In the present study, implants with primary stability had significantly smaller bone level changes than implants with a torque <30 N∙cm, independently of the bone quality of the implant bed and the localization (maxilla or mandible). To date, no other studies have demonstrated a relationship between primary stability and bone level changes.
The time point for the most effective implantation in the context of bone augmentation procedures has been discussed in the literature [837]. In cases when primary stability cannot be guaranteed, it is advisable to perform bone augmentation procedures first, before inserting the implant. However, a reason for the simultaneous approach is the option of direct loading and the concomitant opportunity to reduce bone resorption.
In a literature review, Javed and Romanos [35] highlighted the importance of good primary stability in order to carry out immediate loading regimens. Nonetheless, early implant placement harbours the risk of implant loss due to early wound infection/dehiscence as well as impaired bone healing due to non-vascularised bone grafts. A delayed approach allows re-vascularisation of the bone graft with better regenerative capacity and a higher chance of enhanced osseointegration [7].
To our knowledge, no study has tested the difference between simultaneous and two-stage implantation of dental implants after particulated bone grafting of the posterior mandible. Staged implantation is associated with less bone loss at the mesial and distal sites of the dental fixture than occurs after simultaneous implantation. Moreover, it is important to note the difference in the total number in both of our loading regimens. Further studies focussing on different loading protocols are required to demonstrate the impact of particulated bone grafts on bone resorption.
In order to prevent the dispersion of bone particles and avoid soft tissue ingrowth, barrier membranes were used. In dental bone regeneration, various barrier materials can be applied to prevent the ingrowth of non-osteogenic soft tissue [138]. In addition to non-resorbable membranes, such as titanium mesh and polytetrafluoroethylene membranes, resorbable membranes such as collagen membranes can be used [38]. Here, with consideration of the different sample size (total number of resorbable and non-resorbable membranes used), the utilisation of barrier membranes (resorbable as well as non-resorbable) during the augmentation procedure or the omission of any membrane material did not have any impact on mesial or distal bone resorption.
The results of the present study additionally demonstrated that peri-implant bone changes were influenced by chronic nicotine abuse, although this effect was not statistically significant. A recent meta-analysis has reported a correlation between implant failure and chronic nicotine abuse [39]. However, no studies have addressed peri-implant bone changes after particulated bone grafting in the context of chronic nicotine abuse.
The results of the present study demonstrated that patient age did not have an impact on peri-implant bone loss. Similar observations were presented by Fretwurst et al. [27] after augmentation procedures with iliac bone grafts. Regarding gender, smaller bone level changes were found in females than males, but this difference was not statistically significant. Only limited data have been reported in the literature about the influence of gender on peri-implant bone loss after augmentation procedures. Interindividual hormone status may influence the bone physiology in autologous bone grafts, but further studies are necessary to refute or confirm this possibility. To date, no data have been reported about the influence of hormone levels on peri-implant bone loss in the aging population.
 XML Download
XML Download