

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periodontitis is a multifactorial disease that is primarily caused by subgingival communities of bacteria such as Porphyromonas gingivalis, Actinobacillus actinomycetemcomitans, and Bacterium forsythus [1]. These periodontal pathogenic microorganisms can cause direct damage to the periodontium or indirectly trigger host immune inflammatory responses leading to the loss of connective tissue attachment and alveolar bone and eventual tooth loss [2]. Classic research studies demonstrated that scaling and root planing (SRP), which is an anti-infective procedure, can reduce bacteria supra-gingivally and sub-gingivally and is effective for the treatment of periodontitis [345]. However, the limitations of local anatomical factors [345] and poor host resistance [67] can restrict the effectiveness of periodontal repair following SRP. Even if inflammation is controlled and the progressive bone loss is effectively stopped, the complete regeneration of functional periodontal tissue is still limited.
Most of the destruction of the extracellular matrix of the gingiva and bone in periodontitis is caused by the direct action of host-derived cytokines, enzymes, and some other mediators [7]. The host response is believed to play an essential role in the breakdown of connective tissue and alveolar bone loss, which are key features of the disease process [8]. Therefore, the use of anti-resorptive drugs to control and modulate the host response may provide an effective adjuvant therapy to stimulate the regeneration of lost periodontal tissue [9]. Bisphosphonates are structurally similar to pyrophosphate, which is a component of human metabolism and they are known to inhibit osteoclastic bone resorption [10]. These molecules exhibit highly specific binding to the Ca2+ ions of hydroxyapatite crystals which prevents them from being dissolved by interfering with osteoclast function [11]. This property has led to their use in the treatment of various diseases associated with increased bone resorption, such as osteoporosis, Paget disease, and hypercalcemia caused by malignancies or estrogen deficiency [12131415]. Alendronate is a novel bisphosphonate that contains a terminal amino group and is classified as an aminobisphosphonate [16]. Due to its ability to influence osteoblasts, osteoclasts, its anti-inflammatory [13], and antimicrobial properties [17], several animal and clinical studies have been performed to investigate whether alendronate has a beneficial influence on tissue reparation in periodontitis. However, the quality of these trials varied tremendously, the sample sizes were small, and the results were also inconsistent. Its effectiveness still remains to be established, and to date, no relevant systematic quantitative evaluations using a meta-analysis approach have been performed.
Therefore, the objective of our study was to conduct a meta-analysis to evaluate the effectiveness of adjunctive alendronate for the treatment of periodontitis compared with SRP alone in terms of clinical and radiographic parameters.
MATERIALS AND METHODS
Search strategy
Searches were conducted in the electronic databases PubMed, EMBASE, the Cochrane Central Register of Controlled Trials, the Cochrane Database of Systematic Reviews, Web of Science, and Science Direct, including results published as of September 26, 2016. For the PubMed library, combinations of controlled terms (MeSH and EMTREE) and keywords were used whenever possible. To minimize potential reviewer bias, 2 reviewers (Jin Chen and Qian Chen) designed and assessed the proposal for the present project to ensure that the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [1819] were followed during the screening process. PubMed was searched using the following search format with Boolean operators and an asterisk (*) as a truncation: (“Periodontitis” [Mesh] OR “Periodontal Diseases” [Mesh] OR “Periodontal Pocket” [Mesh] OR “Periodontal Attachment Loss” [Mesh] OR periodontitis OR periodontal disease* OR periodontal osseous defects OR periodontal pocket* OR pocket depth OR attachment loss OR clinical attachment level OR alveolar bone loss OR bone defect fill OR bone defect depth OR periodontal non-surgical treatment OR periodontal non-surgical therapy OR scaling root planing OR dental scaling OR periodontal treatment OR periodontal therapy OR calculus remov* OR calculus debridement OR dental debridement OR periodontal debridement OR “Dental Scaling” [Mesh] OR “Root Planing” [Mesh] OR “Dental Prophylaxis” [Mesh]) AND (Alendronate [Mesh] OR Alendronate OR ALN). The retrieval methods for the other databases were adjusted appropriately based on the above terms.
Inclusion and exclusion criteria
Studies were included if they were randomized controlled trials (RCTs) conducted in humans who were diagnosed with periodontitis that compared SRP with alendronate to SRP alone and included a follow-up period of at least 6 months. Studies were excluded if they incorporated surgical periodontal treatment and/or the use of alendronate in combination with an additional regenerative bone graft material.
Data extraction and quality assessment
Data were extracted by 2 independent reviewers (Jin Chen and Qian Chen). Disagreements were resolved through discussion to reach a consensus. The data from the papers that met the selection criteria were extracted and processed for analysis. The following data were extracted from the included studies: study design; periodontal disease type; health status; study population; number, gender, and age of participants; type of intervention; adverse events; important outcomes; and length of follow-up.
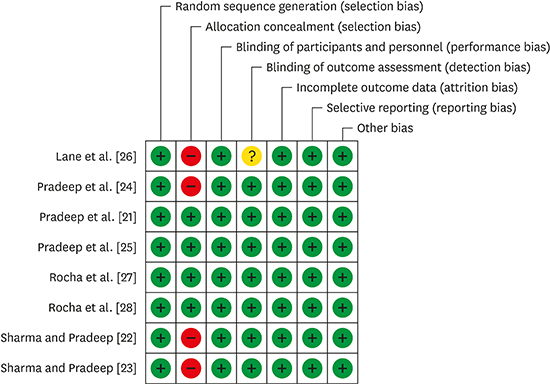
Quality assessment of the studies was performed by focusing on the methodological topics highlighted by Higgins and Green [20] in the Cochrane Collaboration tool for assessing the risk of bias. Using this approach, we assessed the following 7 issues in RCTs: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, handling of incomplete outcome data, selective outcome reporting, and other sources of bias. A low risk of bias was assigned if all criteria were met, a moderate risk of bias was assigned if 1 of these 7 criteria was not satisfied, and a high risk of bias was assigned if 2 or more of these criteria were not satisfied.
Statistical analysis
A meta-analysis was performed using the Review Manager 5.3 software (RevMan Version 5.3 for Windows, the Nordic Cochrane Centre, the Cochrane Collaboration, Copenhagen, Denmark) by 2 authors (Jin Chen and Qian Chen). The results were estimated and reported as mean differences (MDs) with 95% confidence intervals (CIs). Either a fixed-effect or a random-effect model (in the presence of heterogeneity) was used to calculate the overall effect size. The level of significance was set at P<0.05. Heterogeneity between the studies was tested and evaluated with the Q and I2 tests with significance set at P<0.1. However, due to the moderate insensitivity of the Q statistic, only an I2 value lower than 50% was considered a reliable indicator of the absence of heterogeneity [20]. If heterogeneity existed, subgroup analyses were performed according to variance in health status (health or diabetes mellitus) and disease patterns (chronic periodontitis, aggressive periodontitis, or furcation defects). We also conducted a sensitivity analysis using STATA (Version 12.0, Stata Corp., College Station, TX, USA) to explore the stability of our results. Publication bias was not assessed by a funnel plot in our meta-analysis due to the small number of studies. It was likewise not possible to use the Begg test and Egger test for publication bias due to insufficient statistical power resulting from the inclusion of fewer than 10 studies [20].
RESULTS
Study selection
Initially, 483 non-overlapping titles were identified in the electronic search. After the exclusion of duplicates, 293 articles were selected. Titles and abstracts were screened by 2 reviewers and the full text of the remaining 14 articles was then obtained. Based on a careful reading of the full-text articles, 6 articles were excluded. The full text of the remaining 8 articles [2122232425262728] was analyzed for methodological quality and the availability of data for the meta-analysis. Finally, these 8 studies were identified as meeting the criteria for inclusion in this meta-analysis. The main characteristics of the 8 included studies are summarized in Table 1. A flowchart for the study selection process is given in Figure 1.
Table 1
Characteristics of the included studies (n=8)

| Reference | Study design, blinding | Location | Subjects' health status | Participants (sites) | Gender/age (yr) | Smokers | Intervention | Adverse events | Outcomes and follow-up |
|---|---|---|---|---|---|---|---|---|---|
| Pradeep et al. [25] | RCT, parallel, double-blind | India | Chronic periodontitis, healthy | 104 (104) | 53 M, 51 F/30–50 | No smokers | Test 1: SRP+L1 | No adverse events | PD, CAL (0, 3, 6, and 9 months); DDR% (6 and 9 months) |
| Test 2: SRP+L2 | |||||||||
| Control: SRP+placebo | |||||||||
| Pradeep et al. [21] | RCT, parallel, double-blind | India | Class II furcation defects, healthy | 69 (69) | 37 M, 32 F/30–50 | No smokers | Test: SRP+L1 | No adverse events | PD, CAL (3, 6, and 12 months); bone defect fill (6 and 12 months) |
| Control: SRP+placebo | |||||||||
| Sharma and Pradeep [22] | RCT, parallel, double-blind | India | Chronic periodontitis, healthy | 73 (73) | 39 M, 34 F/30–50 | No smokers | Test: SRP+L1 | No adverse events | PD, CAL (0, 2, and 6 months); bone defect fill (0 and 6 months) |
| Control: SRP+placebo | |||||||||
| Sharma and Pradeep [23] | RCT, parallel, double-blind | India | Aggressive periodontitis, healthy | 20 (62) | 12 M, 8 F/20–35 | No smokers | Test: SRP+L1 | No adverse events | PD, CAL (0, 2, and 6 months); bone defect fill (0 and 6 months) |
| Control: SRP+placebo | |||||||||
| Pradeep et al. [24] | RCT, parallel, double-blind | India | Chronic periodontitis, type 2 diabetes mellitus | 43 (78) | 23 M, 20 F/30–50 | No smokers | Test: SRP+L1 | No adverse events | PD, CAL (0, 2, and 6 months); bone defect fill (0 and 6 months) |
| Control: SRP+placebo | |||||||||
| Lane et al. [26] | RCT, parallel, double-blind | USA | Chronic periodontitis, healthy | 66 (9,774) | 37 M, 29 F/Mean age: Test: 48.2±12.8, Control: 46.8±11.5 | 80.3% smokers | Test: SRP+S1 | Test: 87% | PD, CAL (0, 6, and 12 months) |
| Control: SRP+placebo | Control: 68% | ||||||||
| Rocha et al. [28] | RCT, parallel, double-blind | Mexico | Chronic periodontitis, at least 1 year postmenopausal | 40 (unknown) | 40 F/55–65 | No smokers | Test: SRP+S2 | No statistical analysis | PD, CAL (0 and 6 months) |
| Control: SRP+placebo | |||||||||
| Rocha et al. [27] | RCT, parallel, double-blind | Mexico | Chronic periodontitis, type 2 diabetes mellitus | 40 (unknown) | 20 M, 20 F/50–60 | No smokers | Test: SRP+S2 | No statistical analysis | PD, CAL (0 and 6 months) |
| Control: SRP+placebo |
RCT, randomized controlled trial; SRP, scaling and root planing; L1, local delivery of 1% alendronate gel; L2, local delivery of 1.2% atorvastatin gel; S1, systemic administration of alendronate (10 mg/day) or risedronate (5 mg/day); S2, systemic administration of alendronate (10 mg/day); PD, probing depth; CAL, clinical attachment level; DDR%, defect depth reduction.

Characteristics and quality assessment of the included studies
The 8 RCTs included in the study compared SRP with alendronate to SRP with placebo for the treatment of patients with periodontitis. All studies used parallel, double-blinded, and placebo-controlled designs. A follow-up period of 6 months was included in all articles. All studies reported measures of probing depth (PD) reduction and clinical attachment level (CAL) gain, and 5 studies also reported bone defect fill gain in response to local drug delivery.
The quality assessment values are presented in Figure 2. Allocation concealment was adequate in 4 articles [21252728] and was not mentioned in the other 4 included articles. Detection bias was also not mentioned in 1 study [26]. The rest of the quality assessment values were considered adequate in all included trials. Based on a summary of these criteria, the estimated potential risk of bias was low in 4 studies [21252728] whereas the other 3 [222324] showed a moderate risk of bias and 1 showed a high risk of bias [26].

Meta-analysis
Bone defect fill
The results of the meta-analysis revealed that patients who received SRP with local alendronate showed significantly greater improvements in bone defect fill from baseline to 6 months of follow-up than patients who received SRP with placebo. The MD of the bone defect fill improvement was 38.25% (95% CI=33.05–43.45; P<0.001; Figure 3) and substantial heterogeneity was observed (P<0.001; I2=94.0%).
Figure 3
Forest plot from random effects of meta-analysis evaluating the difference in percentage of bone defect fill 6 months after SRP treatment with local alendronate.
SRP, scaling and root planing; SD, standard deviation; CI, confidence interval; IV, inverse variance method.

In our subgroup analysis, the overall effects of local alendronate according to different health statuses (bone defect fill, I2=79.1%; Figure 4) and the disease types (bone defect fill, I2=97.1%; Figure 5) showed high degrees of heterogeneity between studies.


Probing depth
Significant differences were found for PD reduction in locally and systemically administrated alendronate. The MD of PD reduction was 2.29 mm locally (95% CI=2.07–2.52; P<0.001; Figure 6) and 0.36 mm systemically (95% CI=0.18–0.55; P<0.001; Figure 7). The presented data did not show a significant level of heterogeneity in the changes in PD locally (P=0.930; I2=0.0%) or systemically (P=0.450; I2=0.0%).


Clinical attachment level
Significant differences were found in CAL gain between locally and systemically administered alendronate. The MD of CAL gain was 1.92 mm locally (95% CI=1.55–2.30; P<0.001; Figure 8) and 0.39 mm systemically (95% CI=0.11–0.68; P<0.001; Figure 9). Substantial heterogeneity was found in the changes in CAL after local administration (P<0.001; I2=66.0%), but not after systemic administration (P=0.340; I2= 6.0%). The overall effects of local alendronate in all of the subgroup analyses showed a low degree of heterogeneity (CAL, I2=0.0%; Figures 10 and 11) among the studies.
Figure 8
Forest plot from the random-effect meta-analysis evaluating the difference in CAL gain 6 months after SRP treatment with local alendronate.
CAL, clinical attachment level; SRP, scaling and root planing; SD, standard deviation; CI, confidence interval; IV, inverse variance method.

Figure 9
Forest plot from the random-effect meta-analysis evaluating the difference in CAL gain 6 months after SRP treatment with systemic alendronate.
CAL, clinical attachment level; SRP, scaling and root planing; SD, standard deviation; CI, confidence interval; IV, inverse variance method.



Sensitivity analysis
Substantial heterogeneity can be seen in Figures 3 and 8 (I2=94.0% and I2= 66.0%, respectively). To explore the stability of the results across studies, we performed a sensitivity analysis. The overall effect size of the results did not change significantly after repeatedly excluding a single trial in turn from the analysis, which suggested that the results were statistically stable and reliable (Figures 12 and 13).

DISCUSSION
Due to its ability to modulate the host response and inhibit the action of osteoclasts, alendronate has been well received by periodontal practitioners as a promising adjunctive technique with SRP for the treatment of periodontitis. It has been shown that locally delivered alendronate with SRP was more effective in the treatment of periodontitis than SRP alone. However, some previous publications have presented inconsistencies in the effectiveness of systemic alendronate as an adjunct to non-surgical treatment; some showed that systemic alendronate as an adjunctive treatment improved clinical outcomes, while others did not [262728]. Therefore, a systemic assessment of the literature on this subject is needed.
Our meta-analysis showed that locally delivered alendronate with SRP, compared with SRP alone, significantly increased bone defect fill increase by 38.25% (95% CI=33.05%–43.45%), reduced PD by 2.29 mm (95% CI=2.07–2.52 mm) and increased CAL by 1.92 mm (95% CI=1.55–2.30 mm). In addition, systemically administered alendronate with SRP, compared with SRP alone, significantly reduced PD by 0.36 mm (95% CI=0.18–0.55 mm) and increased CAL by 0.39 mm (95% CI=0.11–0.68 mm). These findings show that both the local and systemic utilization of alendronate could improve the efficacy of SRP in patients with periodontitis. However, it should be emphasized that although alendronate has a good safety record, recent reports indicate that systemic alendronate may have some side effects, such as osteonecrosis of the jaws [29]. Thus, when considering the use of systemic alendronate therapy, its potential dangers should also be kept in mind.
Over the years, studies on the mechanisms of action of alendronate have characterized its modulation of periodontal hard and soft tissue healing. In hard tissue healing, it primarily inhibits the receptor activator of nuclear factor kappa B (RANK) signaling pathway and macrophage colony-stimulating factor (M-CSF) expression, leading to reduced osteoclast formation and bone resorptive capacity [30]. In soft tissue healing, it acts as a wound-healing enhancer with anti-inflammatory and antimicrobial biological properties. On one hand, the reduction of neutrophil infiltration in the inflamed gingivae and the release of proinflammatory cytokines such as interleukin-6 and matrix metalloproteinase may reduce the soft tissue lesions [31]. On the other hand, the reduction of the periodontal pocket and direct antibacterial activity may also contribute to the antibacterial activity of alendronate [1731]. This biological mechanism provides plausible evidence for the effect of alendronate on wound healing in periodontal defects.
The risk of bias and heterogeneity are of utmost importance when conducting a meta-analysis of the literature. Four of the studies we included were considered to have a low risk of bias [21252728]. The other 3 studies had a moderate risk of bias based on the descriptions of patient allocations to each group and 1 showed a high risk of bias [22232426]. Formal testing for publication bias could not be performed due to the limited number of articles. The small size of the included trials may underpower this type of analysis; therefore, the risk of publication bias remains possible in this field of research [20]. The substantial level of heterogeneity (I2=94.0% for bone defect fill and I2=66.0% for CAL) in locally delivered alendronate made it prudent to use part of the data as a demonstration of the extent of the differences between therapies. The observed heterogeneity in bone defect fill and CAL among local trials could be attributed to differences in diagnostic criteria, severity of disease, health status, gender ratio, and the number of sites examined in each subject. The subgroup meta-analysis suggested that health status and disease types were not associated with a significant degree of heterogeneity among studies for CAL, but these factors did show a significant degree of heterogeneity for bone defect fill, which may have been responsible for the high heterogeneity among trials. Due to the paucity of studies that were included, we were not able to consider some of these factors further for a subgroup analysis or meta-regression. In the sensitivity analysis, the overall effect size of the results did not change significantly when the meta-analysis estimates were computed by omitting one study in each round, which confirmed the stability of the results. Since all of the results of the included articles were in favor of the conclusion, we were still able to conclude that local alendronate led to additional significant effects on bone defect fill and CAL.
Some limitations of the present study should be recognized. First, only 8 studies were eligible for inclusion in the meta-analysis, and all 5 of the studies on locally delivered alendronate were from the same organization, which limits the generalizability of the results. Second, the original papers did not differentiate between aggressive and chronic periodontitis. Since furcation defects are typically derived from the progression of chronic or aggressive periodontitis and have characteristics that are similar to periodontitis, this disease was also included in our review. Hence, discrepancies in the diagnostic criteria and severity of disease among studies might have influenced the results. Finally, the power of formal tests was limited in this meta-analysis due to the small number of studies, meaning that potential publication bias might have influenced our findings.
In conclusion, the results of this meta-analysis of RCTs provide evidence that both the local and systemic utilization of alendronate as an adjunct therapy to SRP can significantly enhance the therapeutic effectiveness of SRP in treating periodontitis. However, given the limitations of our study, precautions must be exercised when interpreting the results. More definitive multicenter RCTs are needed to assess the effectiveness of alendronate application in periodontitis and to obtain stronger conclusions in this regard.
 XML Download
XML Download