

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In recent decades, dental implants have become a treatment option for edentulous patients. Many studies have examined the long-term success of implants, and patient-related, material-related, and provider-related factors have been found to affect their clinical outcomes. Among the material-related factors, physical characteristics of the implants, such as morphology, dimensions (diameter and length), and surface treatment have drawn attention, since they are relatively easy to modify [123].
The implant surface, which is in direct contact with surrounding bone tissue and facilitates osseointegration, is one of the most important controllable determinants of the success of implant placements. Therefore, various surface treatments capable of enhancing osseointegration between implant and bone tissue have been developed and clinically tested.
A synthetic bone graft material, hydroxyapatite (HA; Ca10(PO4)6(OH)2), is an osteoconductive calcium phosphate mineral present in hard tissues, such as bone and teeth, with a high affinity for bone. Studies have shown that the use of plasma-sprayed HA coatings on implant surfaces promoted osseointegration of the implant into the surrounding bone [14]. Some studies have even suggested that the porous structure of HA resembles the porosity of cancellous bone, and it can therefore act as a therapeutic scaffold for the local delivery of drugs to bone [567]. However, although many studies have reported quicker and more rigid osseointegration in implants with an HA coating, whether this surface treatment is clinically useful remains controversial [89].
The first controversial question relates to the physical properties of the HA coating and the bonding conditions of the titanium surface of the implant. When HA is plasma-sprayed onto the titanium surface, the bonding strength of the HA with titanium weakens due to cracks in the HA surface caused by thermal conductivity differences between the metallic surface and inorganic HA [101112]. This fragility and decreased bond strength result in potential fracture points when implants are loaded under significant torque or occlusal forces. Ultimately, these fractures reduce the success of implant placements due to less efficient osseointegration. This weakness, however, is becoming less of an urgent issue as a result of recent achievements in titanium coating technology.
The second point of controversy is that hydrophilic HA coating rough surfaces may induce bacterial aggregation and facilitate the development of peri-implantitis [1011]. This makes HA-coated implants potentially vulnerable to bacterial infections. Therefore, many HA surface treatments in dental implants start 2 to 3 threads below the crest module, rather than directly under it. Since the occlusal loads are mainly concentrated on the crest module and apical region of implants, HA coating immediately under the crest module could potentially improve the longevity of implants by providing superior osseointegrative characteristics.
The implants used in this study were treated with one of 2 types of HA coating. Partially HA-coated implants were treated with a hybrid coating containing HA and resorbable blast medium (RBM), with the HA crystallinity higher than 98%. The RBM surface included 2 mm of the upper fixture, and the rest of the surface was coated with HA to improve the response in the cancellous bone, restrict deposits of bacteria, and reduce marginal bone loss. The Ca:P ratio of the HA surface was 1.76. The surface roughness was Ra=3.0–3.5 μm. In the fully HA-coated implant, the entire surface was coated with HA alone.
Although reports have shown high success rates of HA-coated implants in areas with relatively poor bone quality, diverse results have been obtained regarding long-term clinical outcomes and peri-implant conditions. The purpose of this study was to compare and analyze the peri-implant tissue conditions and prospective clinical outcomes associated with 2 types of HA-coated implants: (1) fully HA-coated implants and (2) partially HA-coated implants with RBM on the coronal portion of the threads. If the former type of implant shows promising results, its further application may lead to better long-term clinical results.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB#: E-1302/190-001) and informed consent was obtained from the participants. The patients’ data were collected by reviewing and analyzing their medical records and radiographic examinations.
Sample size determination
In order to evaluate the clinical efficacy of the fully coated HA implants, the power and the significance levels were set to 80% and 5%, respectively.
The null hypothesis was defined as having equivalent mean values of alveolar bone resorption between the fully HA-coated implant (μ1) and the partially HA-coated implant (μ2) groups. The alternative hypothesis was defined as having different mean values, as indicated in the following equations.
Assuming that the intergroup difference (δ) would be >0.5 mm and the variance of bone resorption (σ2) would be (0.8 mm)2, for a statistical significance level of 0.05, Zα would equal 1.96, and for a statistical power of 80%, Zβ would equal 0.84, σ2 would equal 0.8, and δ would equal 0.5. The number of subjects necessary for the study was calculated as follows:
Since approximately 2 implants were placed in each subject, approximately 25 patients were needed in each group, for a total of 50 subjects.
Assuming that the dropout rate would be approximately 20%, the necessary number of subjects was N×(1/0.8)=50×1.25=approximately 64. Thus, each group was assigned 32 subjects.
Patient selection
A total of 75 participants (48 males and 27 females, mean age of 58.7±10.3 years) who received care at the Department of Oral Maxillofacial Surgery of the Seoul National University Bundang Hospital, Korea were screened for a randomized controlled clinical trial. The full exclusion criteria are presented in Table 1, and a total of 11 subjects were excluded for the following reasons: 9 exhibited no evidence of moderate periodontitis, 1 did not submit a consent form, and 1 did not demonstrate sufficient residual alveolar bone. Thus, 64 of the 75 recruits remained for randomization. All remaining patients had chronic periodontitis with moderate crestal bone loss around the edentulous premolar or molar regions. The severity of periodontitis was characterized on the basis of the amount of clinical attachment loss and probing depth (PD) according to the Centers for Disease Control-American Association of Periodontology definition, and only patients with moderate periodontitis were included in the study (Table 2) [13].
Table 1
Inclusion and exclusion criteria for patient selection

Table 2
CDC-AAP case definition of periodontitis (2007)

After randomizing 64 subjects, 11 more patients who withdrew consent (n=9) or were lost to contact (n=2) were excluded from the study. Thus, 53 patients remained in the study, and each of them was treated with one or more of the 2 types of HA-coated implants (Osstem Implant, Seoul, Korea). A total of 71 implants were placed. In group I, 36 partially HA-coated TS III implants were placed, while in group II, 35 fully HA-coated TS III implants were placed. Subsequently, 9 patients dropped out of the study due to a primary implant stability quotient (ISQ) value of <50 (n=6), sinus perforation (n=1), poor bone quality (n=1), or nonspecific pain (n=1). Ultimately, 21 patients in group I (30 implants) and 23 patients in group II (32 implants) were examined and analyzed (Figure 1A and B).

Implant treatment procedures
Depending on the available width of the crestal bone ridge, implants with diameters of 4.5 mm and 5.0 mm were chosen for placement. The implants were 8.5 mm and 10.0 mm in length. During the implant placement surgery, a sinus lift through the crestal approach and minor guided bone regeneration (GBR; with the use of a resorbable collagen membrane) around the implant were performed when the surgeon decided that they were necessary. The crest modules of the implants were placed 0.5 mm below the alveolar ridge, using either a 1-stage or a 2-stage technique. If more than 2 implants were placed at once, diagnostic cast models were used to pre-fabricate the surgical stent. All implants were placed with torque between 30 and 40 N∙cm. The implant-placement protocols and drilling sequence followed descriptions provided in the manufacturer’s surgical manual.
Panoramic and periapical radiographs were taken postoperatively. The sutures were removed 10–14 days after surgery. General medications, such as broad-spectrum antibiotics, nonsteroidal anti-inflammatory drugs, anti-ulcer agents, and 100 mL of 0.1% chlorhexidine via mouth gargling were prescribed for 5 days. If the implant was placed using a submerged technique, a second operation was performed and a healing abutment connection was placed 3 weeks after the first operation in the mandible and 8 weeks after the first operation in the maxilla. In both the submerged and nonsubmerged techniques, the measurement of the secondary ISQ, impression taking, and bite registration were performed 4–5 weeks after implant placement in the mandible and 10 weeks after implant placement in the maxilla. The final prostheses were typically delivered and loaded 3 months after placement in the maxilla and 6 weeks after placement in the mandible. All prosthodontic procedures were carried out by a highly experienced prosthodontist.
Stability measurement
In order to evaluate the stability and clinical outcomes of the implant, primary and secondary ISQ values were measured before prosthesis loading using a resonance frequency analyzer (Osstel Mentor, Ostell, Göteberg, Sweden). Primary stability was measured after an implant was placed at its final depth, and secondary stability was measured immediately before impression taking for prosthesis fabrication. For precision, the mean ISQ value was calculated using values measured at the buccal, lingual, mesial, and distal aspects around a given fixture.
Peri-implant parameters
Peri-implant parameters, including the modified plaque index (mPI), modified sulcus bleeding index (mSBI), and probing depth (PD), were assessed at 4 aspects around the implant 12 months postoperatively [1415]. Peri-implantitis was diagnosed when the peri-implant condition satisfied all three of the following criteria: mucositis with bleeding or suppuration on probing, a PD >5 mm, and progressive crestal bone loss of >5 mm.
Marginal bone loss measurements
Panoramic and standardized periapical radiographs were taken preoperatively and postoperatively to examine the implant sites and their proximal edentulous areas. For both linear and dimensional accuracy of the intraoral radiographs, the paralleling technique using a customized plastic film holding device was used. All radiographs were obtained by 2 experienced radiological technologists who were able to provide good reproducibility.
The baseline intraoral radiographs were taken immediately after surgery, and compared with radiographs taken 12 months after the prosthesis loading in order to observe marginal bone loss differences. Radiographic examinations were inspected independently by a single clinical evaluator to identify any progressive bone loss (Figure 2A and B).
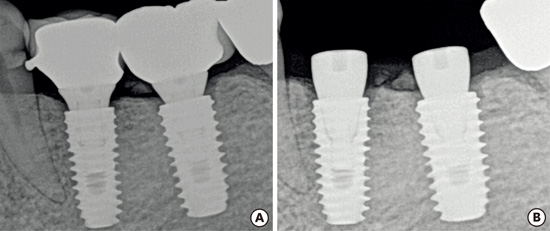
Figure 2
Standardized periapical radiographs. (A) Radiograph taken at the time of provisional crown connection. (B) Radiograph taken 1 year after loading.

Distances between the implant shoulder and the first visible bone-implant contact (mm) were measured using PACS version 3.0.9.1 (INFINITT, Seoul, Korea). The clinician made 2 marks designating where the crestal bone intersected the implant body as shown in the software visualization. The mesial and distal bone loss of the implants were measured to calculate the mean marginal bone loss. Changes in the crestal bone height of each implant were calculated based on the differences between the initial and final measurements made from standardized periapical radiographs. The magnification rate was taken into consideration to compensate for the proportional differences between the real implant length and the length indicated on the radiographs. Each gap between the threads of the implant fixtures was 1 mm, and this known implant dimension was used as a dimensional reference in evaluating the alveolar bone loss observed in radiographs. Measurements were rounded to the nearest 0.01 mm.
Success and survival rates
The success criteria for the osseointegrated dental implants were as follows: (1) no persistent or irreversible subjective pain or complaints, (2) no recurring peri-implantitis infection or suppuration, (3) no perceptible mobility, and (4) no continuous radiolucency around the implant-bone junction [1516]. An implant was also considered a failure if more than 1 mm of bone resorption was found 1 year after the loading (or 0.2 mm/year afterward). If the implants were not physically removed, however, failed implants were included in the survival rate, but not in the success rate [17].
Patient survey (visual analog scale)
In order to measure overall satisfaction levels with the dental implant therapy, all patients filled out questionnaires after the final implant prosthodontic loadings. Satisfaction levels were rated on an 11-point scale, where 10 was the most positive response (completely satisfied) and 0 was the least positive response (completely dissatisfied). The mean overall satisfaction levels were used to evaluate patients’ overall satisfactions with both types of implants.
RESULTS
A total of 62 implants in 44 patients were evaluated. Group I included 21 patients with 30 implants, of which 15 were in the maxilla and 15 were in the mandible, while group II contained 23 patients with 32 implants, of which 19 were in the maxilla and 13 were in the mandible (Figure 3). All implants were placed by an experienced oral and maxillofacial surgeon. The stability and success of the 2 implant types were evaluated throughout routine follow-up examinations, with the duration of follow-up ranging from 3.0 months to 27.6 months (mean, 20.2±6.5 months) for each patient.
Figure 3
Consolidated Standards of Reporting Trials flow diagram of the participants and the implants that were placed.
HA, hydroxyapatite; RFA, resonance frequency analysis; ISQ, implant stability quotient.

The primary and secondary ISQ scores between partially HA-coated (73.1±10.2 and 75.4±7.8, respectively; P=0.153) and the fully-coated implants (69.5±9.2, 73.4±7.0, respectively; P=0.051) did not show statistically significant differences (Table 3). Although this finding was not statistically significant, the fully HA-coated implants showed markedly higher secondary ISQ values than primary ISQ values. Moreover, the fully HA-coated implants did not exert significant negative effects on mucosal health after a year of permanent prosthesis insertion, and they were not associated with a significantly greater risk of peri-implantitis than were the partially HA-coated implants: (mPI: group I, 0.06±0.24 vs. group II, 0.26±0.61; mSBI: group I, 0.26±0.23 vs. group II, 0.51±0.43; and PD: group I, 2.46±0.28 vs. group II, 2.59±0.33; all P>0.05) (Table 4).
Table 3
Mean primary and secondary ISQs (based on RFA values) of partially HA-coated and fully HA-coated implants

| Implant type | n | Primary ISQ | Secondary ISQ | P valuea) |
|---|---|---|---|---|
| Partially HA-coated | 30 | 73.1±10.2 | 75.4±7.8 | 0.153 |
| Fully HA-coated | 32 | 69.5±9.2 | 73.4±7.0 | 0.051 |
| P valueb) | 0.076 | 0.172 | - |
Table 4
Comparison of the soft tissue indices of partially HA-coated and fully HA-coated implants

| Index | Partially HA-coated | Fully HA-coated | P valuea) |
|---|---|---|---|
| mPI | 0.06±0.24 | 0.26±0.61 | 0.120 |
| mSBI | 0.26±0.23 | 0.51±0.43 | 0.949 |
| PD (mm) | 2.46±0.28 | 2.59±0.33 | 0.146 |
In a comparison of the overall annual marginal bone loss (MBL) of the 2 implant types, the partially HA-coated (n=30; 0.33±0.35 mm) and the fully HA-coated implants (n=32; 0.33±0.54 mm) did not show significant differences (P>0.05). The differences were also not statistically significant between the MBL of the maxilla (group I, 0.31±0.33 mm; group II, 0.41±0.67 mm; P>0.05) and the mandible (group I, 0.35±0.39 mm; group II, 0.19±0.19 mm; P>0.05) in both types of implants (Table 5).
Table 5
Mean marginal bone loss in partially HA-coated and fully HA-coated implants

All implants in both implant groups survived, and few partially HA-coated (n=2) and fully HA-coated implants (n=2) showed more than 1 mm of bone resorption 1 year after loading, thereby not fulfilling the success criteria. The survival rate (group I, 100%; group II, 100%) and success rate (group I, 93.3%; group II, 93.8%) of the fully HA-coated implants were not significantly different those of the partially HA-coated implants (Table 6).
Table 6
Survival and success rates of partially HA-coated and fully HA-coated implants

Peri-implant stability can be considerably affected by bone grafts near the crest area. Soft tissue indices and mean marginal bone loss were compared according to the presence of a bone graft in partially HA-coated and fully HA-coated implants (Table 7). Although not significant, the implants with GBR showed less desirable peri-implant conditions than those without GBR. The mean MBL difference in fully-HA coated implants with or without GBR was the only parameter that a showed statistically significant difference (P=0.028). In this case, the mean MBL was much larger in the implants with bone grafting.
Table 7
Soft tissue indices and mean marginal bone loss in partially HA-coated and fully HA-coated implants according to the presence of bone graft

The mean overall satisfaction levels with implant therapy were used to evaluate patients’ overall satisfaction with both types of implants. In both groups, patients indicated that they were highly satisfied (visual analog scores >7), with no visual analog scores <7 indicated (Table 8).

DISCUSSION
Previous studies have shown that the use of HA coatings on implant surfaces can promote the initial osseointegration of implants into the surrounding bone [1011]. Although reports have shown high success rates of HA-coated implants in conditions of relatively poor bone quality, diverse results have been reported for long-term clinical outcomes and peri-implant conditions [1819].
The biocompatibility of HA has been well documented, but its brittleness and relatively low strength has hindered its applications in load-bearing endosseous dental implants [20]. Plasma-sprayed HA surfaces in currently available threaded implants typically start 2–3 threads below the crest module, rather than directly underneath it. This prevents possible fractures caused by differences in thermal conductivity between the titanium surfaces and HA, as well as peri-implantitis induced by hydrophilic HA on rough surfaces [21]. Some researchers have stated that if the rough surfaces of the coronal region of implants come into contact with soft tissues such as the gingiva, complications such as peri-implantitis can arise. In other words, a reliable HA-to-Ti bond is difficult to establish.
The initial dissolution and resorption of the HA coating can cause failures in osseointegration between the implant and bone [3]. Peri-implantitis derived from bacterial contamination could also induce HA-coated implant failures, even if early osseointegration occurs with satisfactory results [10].
According to the criteria introduced by Albrektsson [22], the first month following implant placement is the most important period for osseointegration. If excessive loading on implant fixtures occurs during this period, the equilibrium between bone generation and bone resorption can be broken, resulting in the formation of fibrous connective tissue that could interfere with osseointegration. If the marginal bones are resorbed in the bone-implant interface, the stability of surrounding tissues could be compromised, and eventually peri-implantitis could develop [23].
However, using fully-HA coated implants has considerable benefits, since HA coating directly under the implant crest module may improve the longevity of the implants and promote enhanced osseointegration. This would ultimately provide better implant stability since the occlusal forces are more concentrated on the crest module and apex of the implant. Insufficient stability resulting from shedding of the HA coating and irregular coating thickness has been addressed with technological advancements such as the ion plating and sputtering technique, the thermal decomposition method, and biomimetic processes [23]. Advancements in HA-coating technology could progressively resolve its inherent problems and lead to stable long-term clinical results.
Studies by Berglundh et al. [2425] have provided support for the proposal that smooth implant surfaces are preferable to rough surfaces because they may provide resistance to peri-implantitis as well as a substrate for plaque control and hygiene maintenance. Nonetheless, other researchers have argued that rough treated surfaces, such as RBM and sand blasted with large grit and acid-attacked surfaces, are able to promote good osseointegration without initiating peri-implantitis [26]. In our study, rough surfaces extending to the implant crest module did not exhibit notable weaknesses regarding the prevalence of peri-implantitis (P values >0.05 for all soft tissue indices).
In this study, statistically significant differences were also not found in the annual marginal bone loss of the maxilla (P>0.05) and mandible (P>0.05) for both types of implants. The overall survival rate (group I, 100%; group II, 100%) and success rate (group I, 93.3%; group II, 93.8%) were similar between the fully HA-coated and the partially HA-coated implants. This, in combination with the almost significant increase in the secondary ISQ compared to the primary ISQ in the fully HA-coated implants (P=0.051), shows that if the implants do not fail during the early stages of osseointegration, fully HA-coated implants may promote enhanced osseointegration and have a better chance of implant success.
Of the 9 (of 53) patients who were excluded from further analysis, 6 were excluded due to low primary stability (ISQ <50) (group I, n=4; group II, n=2), and the causes for the exclusion of the remaining patients were sinus perforation (group I, n=1), poor bone quality (group I, n=1), and nonspecific pain (group II, n=1). The clinicians were not able to continue with routine implant therapy in cases of sinus perforation and poor bone quality; therefore, these cases were excluded to eliminate irrelevant variations in surgical procedures. One patient who complained of nonspecific oral pain was also removed from the study since no definite intraoperative problems were found and prosthodontic design could have been the cause of the complaint.
Throughout the study, fully HA-coated implants showed relatively good survival and success rates, as well as primary and secondary stabilities. Overall, a stable and reliable bone level and soft tissue indices were observed in both types of HA-coated implants.
In general, implants with GBR showed less desirable peri-implant conditions than those without GBR. A possible explanation for this is that the graft recipient sites that initially required GBR already had relatively worse periodontal conditions. When soft tissue indices and mean MBL values were compared between the 2 types of HA-coated implants with or without GBR, the only parameter that showed statistical significance was the mean MBL difference in fully HA-coated implants (P=0.028). In this case, the mean MBL was significantly larger in the implants with bone grafts, which may have been due to bonding weaknesses or the hydrophilic properties of HA. Within the limitations of our data, we tentatively suggest that the fully HA-coated implants may have been more strongly influenced by presence of a bone graft.
In conclusion, over the course of a year-long randomized, controlled, clinical trial comparing fully HA-coated and partially-coated implants, the former did not show a significantly greater risk of peri-implantitis, and showed relatively good retention of crestal bone. The present study also showed high survival and success rates in the fully HA-coated implants. In this study, no samples matched the criteria for peri-implantitis, and the observation period of a year was too short to assess the risk of peri-implantitis. Within its limited duration, our study suggests that fully HA-coated implants may be a reliable treatment alternative in edentulous posterior sites, capable of providing good retention of crestal bone.
 XML Download
XML Download