

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Studies have described the placement of implants immediately after tooth extraction. The advantages of this technique include a higher implant survival rate, better aesthetic results, the preservation of alveolar hard and soft tissue volume, and better patient satisfaction due to a shortened treatment period [12345].
Several studies have demonstrated that this protocol cannot reliably preserve the alveolar bone or avoid resorption [6789]. The height of the buccal alveolar bone wall was found to have significantly decreased (2.6 mm loss) 12 weeks after tooth extraction. The residual heights of the buccal and lingual alveolar bone were found to be similar 3 months after simple extraction to those observed after extraction followed by immediate implant placement. The authors of that study observed more bone loss at the buccal wall in both cases [8].
A range of biomaterials, primarily bone xenografts and allografts, have been found to improve osseous volume [10]. In a 30-patient clinical study, the use of biomaterials reduced horizontal loss, but not vertical loss, of the buccal wall [11]. Other studies have demonstrated that vertical bone loss was limited using an allograft covered with a resorbable collagen membrane [1012131415161718]. Clearly, biomaterials delay osseointegration during the time of reossification during new bone-implant contact. The low resorbability of the graft can be clinically considered as an advantage, as it leads to primary stability and limited socket resorption. Allografts that are only osteoconductive have shown comparable results to those of autogenous bone and better results than xenografts, which are mainly used in operations to fill sockets. They have the benefit of avoiding intraoral or extraoral bone harvesting. The reduction of the number of residual cortical particles resulting from the higher rate of resorption of cortical particles compared to xenografts (or bone cancellous allografts) allows the regenerated bone structure to be closer to that of the original bone. Pure cortical allograft particles provide the density and strength of an autograft of cortical bone without the cost or invasiveness of that method. Therefore, the renewed interest of clinicians in allografts, with or without a collagenous membrane, justifies new in-depth studies of this material [131518]. Our study focused on cortical bone chips, which have not been previously studied. The aim of this study was to investigate the benefit of using a mineralized bone cortical allograft, with or without a resorbable membrane, on alveolar bone remodeling after immediate implant placement in a dog model.
MATERIALS AND METHODS
This research protocol was approved by the ethical committee for animal studies of Universidad Autónoma de San Luis Potosí, Mexico. The study was conducted according to the National or Institutional Guidelines for the Care and Use of Laboratory Animals. Six mongrel dogs, approximately 18 months old and weighing approximately 20 kg, were included in this study. During surgical procedures, the dogs were anesthetized with 1 mL/10 kg of intravenously administered tiletamine chlorhydrate and zolazepam chlorhydrate (50/50) (Zoletil 50®, Virbac, Carros, France). Mucoperiosteal full-thickness flaps were elevated to visualize the buccal and lingual hard bone ridge. The teeth were hemisected with the use of a fissure bur and were carefully removed using forceps. Four biradicular premolars (right and left P3 and P4) were extracted from the mandible of each dog, for a total of 48 socket sites (Table 1). Mineralized bone cortical allograft particles treated with Tutoplast® (Puros® cortical, Zimmerdental, Carlsbad, CA, USA) were used for grafting, and collagenous membranes derived from bovine pericardium (Copios®, Zimmerdental) were placed as a barrier to isolate the socket. The control sites were the sockets containing only an implant. The buccal-lingual dimension of the sockets was measured using a sliding caliper after extraction. The following 3 surgical protocols were tested: allograft alone (12 sites), allograft with membrane (24 sites), and control site with implant alone (12 sites). Two types of sockets were evaluated, including intact sockets (S100%; 32 sites; Figure 1A) and sockets with their buccal wall height reduced by 50% (S50%; 16 sites). For the S50% group, the buccal bone wall was reduced with a bur (Figure 1B) and the distance between the buccal alveolar wall and the top of the implant was measured after implantation with a sliding caliper to quantify osseous resorption at the test and control sites, which were randomly selected. Eight implants were placed in each dog in each freshly extracted socket with a marginal level of buccal bone crest. Sockets were prepared for implant installation according to the guidelines provided by the manufacturer. The implants were tapered screw-vent models (Zimmerdental), measuring 3.7 mm wide and 10 mm or 11.5 mm long. Mineralized bone cortical allograft particles were placed to fill the gap around the implant, with or without a collagen resorbable membrane, in order to establish which surgical protocol led to the best results in terms of osseous preservation.
Table 1
Distribution of operations (48 sites, 144 measures)

S50%, socket with buccal wall height reduced by 50%; S100%, intact socket; MBCA, mineralized bone cortical allograft.
![]()
 | Figure 1The 2 types of sockets. (A) Intact sockets (S100%) with 3 implants. The middle implant was placed with cortical Puros® chips (black arrow) in the socket. (B) Sockets with the buccal wall height reduced to 50% (S50%). The implant on the right was cover with mineralized bone cortical allograft (black arrow).
|
The buccal and lingual flaps were managed and secured to allow for submerged healing in the experimental sites. The dogs received 51 mg/10 kg of amoxicillin twice daily (Penamox®, Invekra, Mexico City, Mexico) over 8 days. Dogs were euthanized by an overdose of pentobarbital 1 month after the procedure for 1 dog and 3 months after the procedure for the remaining 5 dogs.
Radiographic analysis
A cone-beam scan (VGi, NewTom, Verona, Italy) was performed for each sample in order to visualize bone resorption and osseointegration and to determine both the direction and position of the implant edges before embedding.
Histomorphometric analysis
The specimens were immediately fixed in 2% glutaraldehyde and 2% formaldehyde in a 0.1M solution of sodium cacodylate buffer at pH 7.4 before dehydration in a graded series of alcohols. The specimens were then embedded in epoxy resin. Undecalcified sections were prepared using an automated ISOMET 2000 (Buehler, Düsseldorf, Germany) precision saw. After polishing, the sections were mounted on glass microscope slides and stained with Goldner trichrome. A Leitz DM-RBE Microscope (Leica, Wetzlar, Germany), associated with a camera D90 (Nikon; Tokyo, Japan), was used for analysis. For each site, 3 histologic sections per site were used for measurements (Table 1).
Histomorphometric measurements
Histomorphometric measurements were completed using Image J (National Institutes of Health, Bethesda, MD, USA). To evaluate osseointegration, bone-implant contact (BIC) was measured on histologic sections (enlargement of ×25). The total length of bone in contact with the implant was measured, and the percentage of the threaded portion of the implant in contact with the bone was calculated. The bone height was calculated by measuring the distance between the buccal or alveolar wall crest and the marginal level of the implant using Image J software on histology sections compared with the measures obtained before the operations.
Statistical analysis
The Shapiro-Wilk normality test showed that the outcome variables (bone height and BIC) were normally distributed. The influence of various surgical parameters on BIC and bone height was analyzed using 4-way analysis of variance with the option of partial sum of squares used for unbalanced data (time, 1 month or 3 months; type of socket, 50% or 100%; allograft, yes or no; and membrane, yes or no). Pairwise comparisons between groups were made using the t-test with Bonferroni correction. Statistical analyses were performed with Stata version 14.1 (Stata Corp., College Station, TX, USA), and the level of statistical significance was set at 0.05.
RESULTS
Histomorphometric analysis
At 3 months, we observed full osseointegration, which would not interfere with grafting and guided bone regeneration operations (Figure 2). The mineralized bone cortical allograft particles were completely embedded in the newly formed bone, which covered almost the entire implant surface (Figure 2). The visualization of residual particles was more difficult at that time. Indeed, the majority of these particles disappeared into the newly formed bone. The particles were sparse and difficult to observe on 25% of the histology sections for all surgical protocols. The observed particles were surrounded with newly formed bone, confirming their capacity for osseoinduction. The internal structure of the particles showed the presence of empty osteocyte lacunae (Figure 3).
 | Figure 2The interface between bone and the implant surface. (A) An implant alone placed into the fresh extraction socket (Goldner trichrome stain). (B) An implant with mineralized bone cortical allograft (Goldner trichrome stain). (C) An implant with a mineralized bone cortical allograft combined with a collagen membrane (Goldner trichrome stain).
|
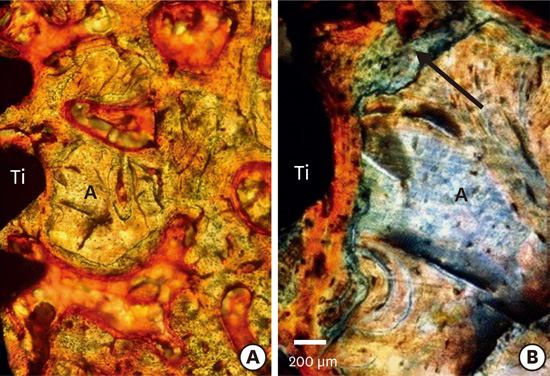
 | Figure 3Interface bone-implant surface with mineralized bone cortical allograft particles without a membrane 3 months after implantation. (A) Mineralized bone cortical allograft (A) and new bone (NB) (Goldner trichrome stain). (B) The black arrow indicates a layer of newly formed bone (B) between the dental implant (Ti) and mineralized bone cortical allograft particles (Goldner trichrome stain).
|
The use of allograft particles significantly reduced buccal wall bone resorption (1.80±2.46 vs. 3.80±1.51 mm) as well as lingual cortical resorption (1.20±1.04 vs. 2.30±0.39 mm). This reduction in bone resorption was higher for the buccal wall than for the lingual wall (Table 2). Finally, the use of a membrane with an allograft significantly reduced buccal wall bone resorption (1.20±2.57 vs. 2.90±2.28 mm). The limited resorption was further reduced to a significant extent when allograft particles were combined with a collagen membrane in comparison to when they were used alone (1.20±2.57 vs. 2.90±2.28 mm for the buccal wall and 1.00±0.78 vs. 1.80±1.07 mm for the lingual wall) (Table 3).
Table 2
Marginal buccal and lingual bone loss with or without allograft particles (cortical Puros®) at 3 months

| Parameter | Bone loss (mm) without MBCA (n=30) | Bone loss (mm) with MBCA (n=30) | P value |
|---|---|---|---|
| BW | 3.80±1.51 | 1.80±2.46 | 0.002a) |
| LW | 2.30±0.39 | 1.20±1.04 | 0.020a) |
Values are presented as mean±standard deviation.
MBCA, mineralized bone cortical allograft; n, number of samples; BW, buccal wall; LW, lingual wall.
a)Statistically significant difference compared to baseline.
![]()
Table 3
Marginal buccal and lingual bone resorption with mineralized bone cortical allograft particles with or without a collagenous resorbable membrane (Copios®) at 3 months

| Parameter | Bone loss (mm) without membrane (n=40) | Bone loss (mm) with membrane (n=40) | P value |
|---|---|---|---|
| BW | 2.90±2.28 | 1.20±2.57 | 0.030a) |
| LW | 1.80±1.07 | 1.00±0.78 | 0.010a) |
Values are presented as mean±standard deviation.
BW, buccal wall; LW, lingual wall; n, number of samples.
a)Statistically significant difference compared to baseline.
![]()
At 1 month, we observed that the buccal and lingual crests were located at 2.10±0.03 mm on the buccal side and 0.40±0.01 mm on the lingual side, apical to the marginal level of the implant, in the S100% sockets. The bone resorption was higher for the buccal and lingual walls at 3 months than at 1 month. This resorption was significantly lower for the buccal wall in the S50% group than in the S100% group, and buccal wall resorption was significantly more extensive (Table 4).
Table 4
Comparison of buccal and lingual bone resorption measured in histological sections for the S50% and S100% sockets after 1 and 3 months in the control sites

Values are presented as mean±standard deviation.
BW, buccal wall; LW, lingual wall; n, number of sites; S50%, socket with buccal wall height reduced by 50%; S100%, intact socket.
a)Statistically significant difference compared to baseline.
![]()
Osseointegration was incomplete at 1 month for all protocols.
At 1 and 3 months, mineralized bone cortical allograft with or without a collagen membrane did not disturb osseointegration in comparison with the control site (Table 5, Figure 2). The mineralized bone cortical allograft was observed 1 month (Figure 4) and 3 months after implantation (Figures 3 and 5). At 1 month, while osseointegration was incomplete, the allograft particles were surrounded by a thin layer of newly formed bone and were therefore never directly in contact with the implant surface. Active resorption areas of allograft particles were visible (Figure 4).
Table 5
Comparison of BIC at 1 and 3 months after surgery

Values are presented as percentages.
BIC, bone-implant contact; n, number of samples; S50%, socket with buccal wall height reduced by 50%; S100%, intact socket; MBCA, mineralized bone cortical allograft.
a)Statistically significant difference compared to baseline.
![]()
 | Figure 4Histological view of a titanium implant 1 month after of implantation. The space between the implant and the alveolar socket was filled with mineralized bone cortical allograft and a membrane was placed in the buccal side. (A) Mineralized bone cortical allograft particles (Goldner trichrome stain). (B, C) Enlarged views of mineralized bone cortical allograft particles. The green layer surrounding the mineralized bone cortical allograft corresponds to newly formed bone. In both cases, contact between newly formed bone and the implant surface was established (black arrows). The newly formed bone layer is continuous around the mineralized bone cortical allograft particles in contrast to the titanium (Goldner trichrome stain).
|
 | Figure 5Bone-implant interface with mineralized bone cortical allograft particles and a membrane 3 months after implantation. (A) General view with mineralized bone cortical allograft particles (Goldner trichrome stain). (B) The black arrow indicates a layer of newly formed bone between the dental implant (Ti) and particles of mineralized bone cortical allograft (A) (Goldner trichrome stain).
|
Indeed, the Tutoplast® processing performed on this material, with the aim of eliminating the risk of contamination through various treatments, allows protection of the collagenic mineral weft and the architecture of the donor. Observation with strong magnification (×400) allows visualization of these residual particles and shows the presence of empty gaps of osteocytes. Furthermore, the Goldner trichrome staining of these particles is different from that of the newly formed bone, due to the chemical modification of the organic matrix during Tutoplast® processing.
X-ray tomography
X-ray tomography scans showed that buccal wall resorption was observed for all surgical protocols and that less resorption was observed in the lingual walls (Figures 6, 7, 8, and 9). Osseointegration was incomplete at 1 month for all protocols (Figure 6). At 3 months, mineralized bone cortical allografts alone or combined with a membrane limited the resorption of the buccal wall and preserved the bone volume. In these situations, the resorption of the buccal wall was limited in height, but losses in bone volume were still observed (Figures 7 and 8). Full osseointegration was observed, which would not interfere with grafting and guided bone regeneration operations (Figures 6, 7, 8, and 9).
 | Figure 6X-ray tomography at 1 month (S100%, intact socket). (A) Mesio-distal view of 3 implants. (B) Linguo-vestibular view of an implant with mineralized bone cortical allograft particles and a membrane. The blue arrow indicates the buccal wall with limited height and widthwise bone resorption.
|
 | Figure 7X-ray tomography at 3 months (S100%, intact socket). (A) Mesio-distal view of 4 implants. (B) Linguo-vestibular view of implant B with mineralized bone cortical allograft particles and a membrane. The blue arrow indicates the buccal wall with limited resorption.
|
 | Figure 8X-ray tomography at 3 months (S100%, intact socket). (A) Longitudinal view of 4 implants. (B) Coronal view of implant C with mineralized bone cortical allograft particles. The blue arrow indicates the buccal wall with post-extraction resorption.
S100%, intact socket.
|
 | Figure 9X-ray tomography at 3 months with 50% of the buccal wall (BW) removed (S50%, buccal wall socket height reduced by 50%). (A) Longitudinal view of 4 implants. (B) Coronal view of implant C with mineralized bone cortical allograft particles and a membrane. The blue arrow indicates the BW with limited resorption.
|
DISCUSSION
The technique of immediately placing implants after tooth extraction does not protect from bone reduction along the buccal-lingual or vertical axes. Alveolar post-extraction resorption varies from 2 to 4 mm in the vertical and horizontal axes, with an average of 3 mm [19]. Certain criteria, including the position of the implant with respect to the crest, the distance that separates the implant from the alveolar buccal wall, and the diameter of the implant, influence bone reshaping during the post-implant healing phase [20]. A study showed that the buccal wall must have an original width of 2 mm to avoid loss of bone height. In addition to the importance of the thickness of the alveolar buccal wall, the space between the implant and socket is also involved in the phenomenon of bone reduction [21]. Indeed, the diameter of a dental root is often larger than the implant. Animal and clinical studies have shown that a space between 1 to 2.25 mm was easily filled after 4 months using rough surface implants with an additional vertical ridge reduction [2223]. A gap between the implant and the socket wall smaller than 1.5 mm will be completely filled independently from the loss in the height of the buccal bone [24].
These data are not significantly different from well-established findings regarding physiological osseous post-extraction resorption.
Our investigation evaluated the dimensional changes (from 1 month to 3 months) of the buccal and lingual alveolar bone wall after placing an implant into fresh extraction sockets (control sites). Post-extraction resorption of the buccal wall was recognized as inevitable in cases of the immediate placement of implants [6782526]. Our results confirmed, in control sites, that immediate implant placement did not avoid post-extraction resorption, regardless of the alveolar bone height, which is in agreement with the current literature [6782021]. At 3 months, dimensional changes of the socket were most pronounced on the buccal side, and greater in magnitude than has been reported in other studies. This tendency was probably related to differences in diet.
Many authors have studied the contribution of regenerative techniques in limiting bone resorption [1012141617192627282930313233343536]. Few studies have assessed mineralized bone cortical allografts in comparison with mineralized or demineralized cancellous allografts or xenografts for the preservation of bone volume and quantity of newly-formed bone. They also showed fewer residual particles in allografts than in xenografts, which contributed to the use of allograft particles in this study [29313738]. Furthermore, we analyzed whether the regenerative procedures associated with these particles influenced bone remodeling around implants.
We observed that dimensional changes in the alveolar ridge occurred following implant placement in fresh extraction sockets, regardless of the application of regenerative procedures, and that buccal wall resorption was more pronounced, both in the control and the test sites.
The findings of this study confirm the positive contribution of these regenerative techniques in terms of osseous volume preservation during implant surgery for both cortical allograft particles (cortical Puros®) and cortical allograft particles combined with a resorbable collagenic membrane (Copios®), with better osseous volume preservation observed when mineralized bone cortical allograft was combined with a collagenous membrane.
This could be explained by the fact that the graft was placed between the implant and buccal wall. When peri-implant gaps were filled with mineralized bone cortical allograft, post-extraction bone resorption was reduced, not prevented completely. Therefore, regenerative procedures (i.e., a mineralized bone cortical allograft combined with a resorbable collagenous membrane) improved bone remodeling and osseointegration around the implants.
Additionally, at 1 month, we observed a significant increase in the BIC when the mineralized bone cortical allograft was used in comparison with the control sites, demonstrating that osseointegration was not perturbed and may instead have been accelerated. Mineralized bone cortical allograft particles did not perturb osseointegration because they were never in direct contact with the implant surface.
In the early period of healing, allograft particles were surrounded by newly formed bone, confirming their capacity for osseoconduction, but they did not form a real continuity with the socket bone. They had a high degree of biocompatibility with the surrounding tissue and were mainly replaced by newly formed bone at 3 months. These observations for residual cortical Puros® chips are similar to those made in studies of other allografts [29363738].
Considerable interest has emerged in bone cortical allograft particles in the immediate extraction-implantation technique. The smaller number of residual particles due to higher resorbability than xenografts or other biomaterials described in the literature allows the regenerated bone structure to be more similar to the original bone. A mineralized bone cortical allograft combined with a collagen membrane allows a significant reduction in buccal and lingual bone resorption, which was higher than observed using mineralized bone cortical allograft alone. The membrane is used as a barrier to hold the mineralized bone cortical allograft in place during the entire healing time. Therefore, the real benefit of using a mineralized bone cortical allograft and membranes in implant surgery is preserving bone volume and enhancing osseointegration, which are the key factors for clinical success.
In conclusion, within the limits of this study, we demonstrated that the regenerative technique after immediate implant placement in a fresh extraction socket with bone cortical allografts combined with a membrane significantly limited buccal wall bone resorption. Furthermore, we showed that when this technique was used, the regenerated bone was similar to the original bone in terms of histological structure.
 XML Download
XML Download