

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
In modern dentistry, patients' demands not only for recovery of lost masticatory function, but also for recovery of dental aesthetics, are ever growing. Particularly in the case of the upper anterior area, the patient's aesthetic demands can be met when restorations are made such that the gingival topography matches the gingival contour. However, creating natural-looking soft tissue in the upper anterior area is a difficult task [1]. The criteria for successful soft tissue formation in the upper anterior area largely rely on the existence of a healthy interdental papilla and the formation of a matching gingival contour [2]. A deficiency in interdental papillae creates problems with pronunciation and food impaction, along with aesthetic issues [3]. Interdental papillae not only play a role in protecting the periodontal tissue in the upper anterior area by blocking food impaction, but also serve an aesthetic purpose [4].
To date, many studies have analyzed the factors influencing deficient interdental papillae. Among such studies, the study by Tarnow et al. [5] reported that interdental papillae were often present when the distance between the contact point and the bone crest (CP-BC) was ≤5 mm. Moreover, in a study by Cho et al. [6] on the effects of the interproximal distance between roots (IDR) on the presence of interdental papillae, according to the CP-BC, it was reported that, as IDR or CP-BC increased, the interdental papillae were less frequently present. In particular, when the CP-BC was 4–6 mm, an increase in the IDR resulted in a sensitive decrease in the presence of interdental papilla. Unlike the study by Tarnow et al. [5], which included both the anterior and posterior areas, Chen et al. [7] conducted a study on only the upper anterior area and reported that, when CP-BC was ≤4 mm, interdental papillae were present in 100% of the cases, whereas when this distance was ≥7 mm, interdental papillae were always deficient. Although other studies have reported that gender, interproximal embrasure area, interdental papilla length, and crown morphology are associated factors [8910], CP-BC is considered the most important associated factor for the presence of the interdental papilla [5678910].
Various periodontal plastic surgery methods have been suggested for the reconstruction of deficient interdental papillae. Although a variety of surgical procedures and flap designs have been suggested [1112131415], they have had limited success and have lacked predictability; as such, interdental papilla reconstruction is considered one of the most challenging periodontal plastic surgery procedures [15]. Therefore, aesthetic enhancement of deficient interdental papilla requires the use of aesthetic restorative resin, prosthetic restoration, or an orthodontic approach. However, Becker et al. [16] used commercial injectable hyaluronic acid gel for deficient interdental papillae in a small area, the first report to show that minimally invasive and predictable reconstruction of deficient interdental papillae was possible. Hyaluronic acid is a member of the glycosaminoglycan family and a major component of the extracellular matrix in almost all tissues. Its primary role is to bind water to maintain tissue structure and its characteristics, including consistency, biocompatibility, and hydrophilicity, have made it an excellent moisturizer in cosmetic dermatology and skin-care products. To date, injectable hyaluronic acid gel has been successfully used to reduce wrinkles and improve other similar facial deformities [17].
Accordingly, the present study aimed to investigate the effects of hyaluronic acid gel injection for the reconstruction of deficient interdental papillae in the upper anterior area, using an image analysis system to assess the clinical and radiographic factors influencing reconstruction of the interdental papilla by means of this procedure.
MATERIALS AND METHODS
Patient selection
The present study was conducted with approval from the Institutional Review Board of Chosun University Dental Hospital (CUDHIRB-1501-002). All participants in the study were provided with an overview of the clinical trial and explanations of patient guidelines and relevant information were given; the study was conducted after signed consent forms were obtained from each participant.
Among the patients of Chosun University Dental Hospital, a total of 13 patients, 6 male and 7 female patients, were recruited. Participants' ages ranged between 27 and 35 years, with a mean age of 32 years. The inclusion criteria included patients with at least 1 papillary deficient site in the upper anterior area and with a plaque index [18] and gingival index [19] between 0 and 1. Patients who were pregnant, patients taking medication known to increase the risk of gingival enlargement, and those who were currently receiving orthodontic treatment on the upper anterior area were excluded.
The experiment was conducted on a total of 65 sites in the upper anterior area with papillary deficiency. Among these sites, 5 sites were excluded, since the black triangle area was too small to be measured via an image analysis program, while 3 sites were excluded because of the absence of contact points due to the presence of diastema. Consequently, the study was conducted on a total of 57 sites in the upper anterior area with papillary deficiency.
Procedure
The study models were prepared from the upper impressions acquired during the initial examination, which were used to create the clinical photographic and periapical radiographic standardization devices (Figure 1). If the horizontal and vertical angles change during clinical imaging of the same area with a papillary deficiency between time points, the black triangle area can be distorted. Therefore, the clinical images at the initial examination and 6 months later were taken using a brown-colored round post that does not show on the images, to ensure consistency in image composition and to minimize errors in future imaging analysis measurements of the black triangle area. Moreover, a periapical radiographic standardization device with 5-mm wires attached horizontally and vertically was designed and used as a standard to determine actual changes in length on radiographic images.

The surgical procedures were as follows. The single injection dose from the injection-assistance device (CelTick®, Hyundae Meditech, Wonju, Korea) was set to 0.002 cc. The injectable hyaluronic acid gel (Teosyal Puresense Global Action®, Teoxane, Geneva, Switzerland) and disposable 30G×1/2" needle (Jungrim Medical, Seoul, Korea) were then loaded. The needle was inserted at a 45° angle, 2–3 mm apical to the involved papilla [16]. A single-point injection technique was employed, and the bevel of the injection needle was applied sloping upward. Each involved papilla was injected with a total of 0.01 cc by injecting 0.002 cc of hyaluronic acid gel each time, for a total of 5 times, in order to prevent any flow-back of the hyaluronic acid gel due to periodontal tissue pressure. Subsequently, the involved papilla was molded by reconstruction in the incisal direction using gauze to apply light pressure. This method was repeated up to 5 times, at 3-week intervals, until the black triangle was no longer clinically observable. The final clinical photographs and periapical radiographic images were taken at 6 months after the initial procedure.
Outcome measurements
The values for 3 variables-black triangle area (BTA), height (BTH), and width (BTW)-were measured from clinical photographs taken during the initial examination and 6 months later, using an image analysis program (Adobe Photoshop CS5®, Adobe Systems Inc., San Jose, CA, USA) (Figure 2). The measurement of BTA was defined as the number of pixels included in the designated area, while BTH was defined as the difference between maximum and minimum y-axis values, and BTW as the maximum and minimum x-axis values. First, we adjusted the contrast of the photograph to be measured to ensure that the borders of the black triangle were distinct and the physical length of the image was calculated in pixels. Furthermore, pixel values on the clinical photograph equivalent to a periodontal probe length of 10 mm were used as a reference for converting the variable values expressed in pixels to physical length (in mm). The portion of the black triangle that was measured was demarcated on the image and BTA, BTH, and BTW were automatically converted to millimeters. A single assessor with no knowledge of the procedures took all of the measurements, and the mean value for each site was calculated from 10 measurements taken at each site.

In addition, after fitting the periapical radiographic standardization device onto the patient's upper anterior area, periapical radiographic images were acquired from each interdental papilla region. All periapical radiographic images were acquired using a parallel technique by a single trained radiologist. Values for the variables CP-BC, defined as the distance between the contact point and the bone crest, and IDR, defined as the interproximal distance between roots [6], were measured using a radiographic measurement program (PiViewStar 5.0.9.2®, Infinite Healthcare, Seoul, Korea), while the length values were adjusted relative to the 5-mm wire length (Figure 3). A single assessor with no knowledge of the procedures took all the measurements from the periapical radiographic images and the mean value for each site was calculated from 10 measurements taken at each site.
Figure 3
The radiographic analysis. Horizontal and vertical wires of 5-mm length are shown.
IDR, the interproximal distance between roots; CP-BC, the distance between the most apical part of the CP (contact point) and the most coronal portion of the BC (bone crest).

For analysis of the effects of the injectable hyaluronic acid gel, the interdental papilla reconstruction rate (IPRR) was defined as the percentage of change in the initial BTA to the final BTA after 6 months [16].
When the final clinical photographs were taken, cases that showed no clinical signs of a black triangle were categorized into the complete interdental papilla reconstruction (CIPR) group, while cases that still had a clinically observable black triangle were categorized as the partial interdental papilla reconstruction (PIPR) group.
Data analysis
Statistical analysis was conducted using commercially available statistical software (SPSS version 20.2, IBM Corp., Armonk, NY, USA). A Shapiro-Wilk test of normality was done. Mean comparisons of each item between the CIPR group and the PIPR group were carried out using a parametric t-test, while a Mann-Whitney U test was used for nonparametric data. Pearson correlation coefficients were used to determine the relationships of the CP-BC and IDR with the black triangle and IPRR. The Pearson correlation coefficient was also calculated to analyze relationships between CP-BC >6 mm and IPRR. P-values <0.05 were considered to be statistically significant.
RESULTS
After performing interdental papilla reconstruction using injectable hyaluronic acid gel on a total of 13 patients at 57 interdental papilla sites in the upper anterior area, a mean IPRR of 88.80% was found with 3.33 injections, while BTA, BTH, and BTW showed a mean decrease of 0.21 mm2, 0.70 mm, and 0.30 mm, respectively (Table 1).
Table 1
Overall outcomes of interdental papilla reconstruction

ΔBTA, reduction in black triangle area; ΔBTH, reduction in black triangle height; ΔBTW, reduction in black triangle width; IPRR, interdental papilla reconstruction rate; Site A, interdental papilla between maxillary right canine and maxillary right lateral incisor; Site B, interdental papilla between maxillary right lateral incisor and maxillary right central incisor; Site C, interdental papilla between maxillary central incisors; Site D, interdental papilla between maxillary left central incisor and maxillary left lateral incisor; Site E, interdental papilla between maxillary left lateral incisor and maxillary left canine; SD, standard deviation.
CIPR was found in 36 treated sites, while the remaining 21 sites showed an IPRR ranging from 19% to 96%. With respect to comparison of the mean values of clinical and radiographic variables between the CIPR (Figure 4) and PIPR (Figure 5) groups, the initial BTA, BTH, BTW, and CP-BC showed statistically significant differences, whereas the IDR did not show a statistically significant difference between these groups (Table 2).
Figure 4
A case of complete interdental papilla reconstruction. (A) At baseline. (B) At 6 months after reconstruction.

Figure 5
A case of partial interdental papilla reconstruction. (A) At baseline. (B) At 6 months after reconstruction.

Table 2
Comparison between the complete interdental papilla reconstruction (CIPR) group and the partial interdental papilla reconstruction (PIPR) group

IPRR, interdental papilla reconstruction rate; BTA, black triangle area; BTH, black triangle height; BTW, black triangle width; CP-BC, the distance between the contact point and the bone crest; IDR, the interproximal distance between roots; SD, standard deviation.
a)Statistically significant (P<0.05), using the Mann–Whitney U test; b)Statistically significant (P<0.05), using the Student t-test.
As the CP-BC increased, the initial BTA, BTH, and BTW also increased, and were strongly positively correlated (Figure 6A), while the correlation with IDR weakened (Figure 6B).
Figure 6
The correlations among the distance between the contact point and the bone crest (CP-BC), the interproximal distance between the roots (IDR), and the baseline black triangle. (A) Statistically significant positive correlation between CP-BC and the baseline black triangle was observed. (B) No correlation was observed between the IDR and the baseline black triangle.
 , Black triangle area (mm2);
, Black triangle area (mm2);  , Black triangle height (mm);
, Black triangle height (mm);  , Black triangle width (mm).
, Black triangle width (mm).r, Pearson correlation coefficient.
a)Statistically significant (P<0.05).

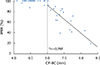
Although the CP-BC showed a statistically significantly strong correlation with the IPRR, there was no statistically significant correlation between the IDR and IPRR (Table 3). For CP-BC up to 6 mm, an IPRR of essentially 100% was observed, while for a value >6 mm, an increase in distance showed a statistically significantly negative correlation with the IPRR (Figure 7).
Table 3
Pearson correlations among the distance between the contact point and the bone crest (CP-BC), the interproximal distance between roots (IDR), and interdental papilla reconstruction rate (IPRR)

| Parameters | CP-BC | IDR | IPRR |
|---|---|---|---|
| CP-BC | 1 | ||
| IDR | −0.141 | 1 | |
| IPRR | −0.864a) | 0.204 | 1 |
Figure 7
The correlation between the distance between the contact point and the bone crest (CP-BC) and the interdental papilla reconstruction rate (IPRR). Two groups were categorized based on a CP-BC cut-off value of 6 mm. A statistically significant negative correlation of CP-BC>6.0 mm and IPRR was observed.
r, Pearson correlation coefficient.
a)Statistically significant (P<0.05).
DISCUSSION
Some studies have already reported that successful interdental papilla reconstruction is possible by using commercial injectable hyaluronic acid gel. In a study by Becker et al. [16], it was possible to achieve 100% CIPR at 3 of 14 sites with a maximum of 3 injections of injectable hyaluronic acid gel at 3-week intervals, while the remaining 11 sites showed an IPRR of 57%–97%. Mansouri et al. [20] used the same experimental methods as Becker et al. [16] and reported a wide-ranging IPRR of 22%–100% at a 6-month follow-up of a total of 21 sites in the upper anterior area, with 9 sites showing an IPRR of ≥50%. In the present study, 52 of a total of 57 sites showed an IPRR of ≥50%. Moreover, CIPR occurred at 36 sites, which is a higher percentage than that reported in other studies, while the remaining 21 sites showed wide-ranging partial reconstruction (19%–96%). These differences may be attributable to differences in the initial interdental papillary deficiency levels and the experimental design. The studies by Becker et al. [16] and Mansouri et al. [20] did not provide information on the initial interdental papillary deficiency levels, making it difficult to make a direct comparison with the results from the present study; however, it is possible that areas with less initial interdental papillary deficiency may have been included in the present study. Moreover, the effect of interdental papilla reconstruction may have been enhanced by more precise injections, made possible by using an injection-assistance device and a 30G needle, as well as the fact that the number of injections was increased to 5, at 3-week intervals.
When the mean values of each variable were compared between the CIPR and PIPR groups, the initial interdental papillary deficiency level and the CP-BC were different to a statistically significant degree. Previous studies [5678910] have reported that the CP-BC was the most important factor in interdental papillary deficiency. Moreover, considering that the deficient area of the interdental papilla also increased as the CP-BC increased in the present study (Figure 6A), it can be surmised that the CP-BC is also an important factor for CIPR using injectable hyaluronic acid gel. However, the present study did not find any association between the initial interdental papillary deficiency level and the IDR (Figure 6B). Earlier studies [69] reported that the presence of the interdental papilla decreased with an increasing IDR, but recent studies [710] have reported that when the CP-BC variable was controlled, the influence of the IDR on the presence of the interdental papilla disappeared. Thus, the IDR has a minimal influence on interdental papilla reconstruction using injectable hyaluronic acid gel.
Interestingly, most cases with a CP-BC of up to 6 mm showed CIPR, but as the distance increased beyond this cut-off, the IPRR tended to decrease (Figure 7). Interdental papillae are generally considered biologically safe and stable with a CP-BC up to 5 mm [7]. Tarnow et al. [5] have also reported that there was virtually no interdental papillary deficiency at a CP-BC ≤5 mm. Injectable hyaluronic acid gel has a predictable interdental papilla reconstruction effect of approximately 1 mm in the vertical direction. Therefore, a CP-BC value of 6 mm can be used as a cut-off value for interdental papilla reconstruction using hyaluronic acid gel.
In the present study, we used a photographic standardization device developed in-house to increase the reproducibility of clinical photographs taken of the interdental papilla areas. In studies by Becker et al. [16] and Mansouri et al. [20], initial photographs were taken perpendicular to teeth of interest and these were used to take subsequent photos as close to the original photos as possible without a special device. Such a method required the utmost effort to reproduce the same horizontal and vertical angles during photography, but we tried to minimize errors in future imaging analysis measurements of the black triangle area by making sure that the brown strip on the cylindrical post was not visible on each clinical photograph acquired. However, although the reproducibility of the photos was improved compared to previous studies, it was still difficult to reproduce a photo at the same corresponding angle (Figures 4 and 5). Therefore, more studies are needed in the development of a more precise reproducible alignment device and method.
Within the limits of this study, the CP-BC was found to be correlated with the BTA, BTH, and BTW, but not with the IDR. Interdental papilla reconstruction using injectable hyaluronic acid gel allowed successful reconstruction when the CP-BC was ≤6 mm, but for the CP-BC >6 mm, the increased distance resulted in a decreased IPRR. Therefore, the CP-BC is closely associated with the efficacy of hyaluronic acid gel injection for the reconstruction of deficient interdental papillae in the upper anterior area.
 XML Download
XML Download