

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Peri-implant mucositis and peri-implantitis can be categorized as biological complications in implant rehabilitation. Peri-implant mucositis has been defined as a reversible inflammatory reaction of peri-implant soft tissues with no radiographic evidence of bone loss [1]. From a clinical perspective, signs that determine the presence of peri-implant mucositis include erythema and swelling, usually associated with probing depths ≥4 mm [23]; however, the essential parameter for diagnosis is bleeding on gentle probing (<0.25 N) [4]. In contrast, peri-implantitis has been identified as a progressive and irreversible infectious pathological condition associated with changes in the level of crestal bone, the presence of bleeding on probing (BOP), and/or suppuration with or without concomitant deepening of the peri-implant pockets around an osseointegrated implant in function [45]. Although these are typical signs, sometimes they are not clearly recognizable. Furthermore, the predictive value of BOP, increased peri-implant probing depth (PPD), or peri-implant bone loss (PBL) as individual features remains insufficiently well established [6]. Despite this, the presence of BOP, PPD, and PBL have been associated with peri-implant lesions when evaluated in the context of specific patient- and site-dependent variables, including age, gender, smoking, adherence to oral hygiene procedures, gingival biotype, the presence of plaque, keratinized tissue and soft tissue recessions, and the type of bone graft and membrane during the implant placement [789]. Etiologically, other factors and conditions may contribute to the development of peri-implant disease, including alcohol consumption, a history of periodontitis, residual cement, bacterial micro-leakage at the implant abutment interface, implant surface characteristics, the type of the prosthetic supra-structure, osteoporosis, and diabetes [1011]. A risk factor has been described as “an environmental, behavioral, or biological factor that, if present, directly increases the probability of a disease (or adverse event) occurring and, if absent or removed, reduces that probability. Risk factors are part of the causal chain, or expose the host to the causal chain,” [12] whereas a risk indicator may be defined as a “probable risk factor that has not been confirmed by carefully conducted longitudinal studies” [12]. Because there is increasing evidence to suggest that peri-implant mucositis is the precursor of peri-implantitis, early detection of risk factors plays a key role in preventing further progression of the disease. Despite the fact that prospective studies are essential to assess true risk factors, retrospective and cross-sectional studies may be suitable to identify risk indicators for the disease [13]. However, it is difficult to compare the analyses of such risk indicators due to heterogeneity between studies in terms of the peri-implant disease diagnostic criteria, the definitions of implant success, and the reference points for measuring the marginal PBL [57]. Consequently, the influence of potential clinical predictors on the diagnosis and prognosis of peri-implant disease might be inadequately reported. Therefore, the purpose of the present retrospective study was to evaluate how the presence of different independent implant- and patient-related risk indicators might influence the odds of developing a peri-implant disease in a randomized cohort of patients.
MATERIALS AND METHODS
Study design and participants
The study reports on patients treated in a university setting with conventional-length (>6 mm), non-turned, 2- and 3-piece titanium implants during a period ranging from 2000 to 2012. A random sample was enrolled of partially and fully edentulous patients with at least one implant-supported restoration in occlusal loading during the appointment for evaluation. The patients were consecutively included, and the data were collected from July 2014 to July 2015 during regular implant maintenance visits. Implant surgical operations and prosthetic restorations were all performed in the same department (Implant Center for Edentulism and Jawbone Atrophies, Maxillofacial Surgery and Odontostomatology Unit, Fondazione IRCCS Cà Granda, Ospedale Maggiore Policlinico, Milan, Italy). To exclude possible operator-dependent bias, clinical measurements were taken by a single blinded investigator. Each patient was given a detailed description of the procedure, and informed consent was obtained prior to participation in the study. The present cross-sectional study was carried out in accordance with the Declaration of Helsinki of ethical human research practices. No ethics committee approval was sought due to the retrospective nature of the present study, and such oversight was not required by national law or by ordinance of the local inspection authority.
Exclusion criteria
In accordance with Konstantinidis et al. [9] and Schwarz et al. [8], for patient selection, the following exclusion criteria were defined: (1) any uncontrolled systemic diseases that could influence the implant therapy outcome (e.g., diabetes [HbA1c >7], osteoporosis); (2) any intake of medications that may have an effect on bone turnover and mucosal healing (i.e., steroids, antiresorptive therapy); (3) any antibiotic treatment for a medical or dental reason within the 2 months prior to the examination; (4) any restorations that did not allow for the calculation of PPD; (5) inability or refusal to sign the informed consent form; (6) fewer than 12 months of follow-up post loading; (7) pregnancy or breastfeeding in women; and (8) the absence of baseline radiographs taken at the time of placement of the suprastructure.
Anamnestic data and implant site characteristics
The following study variables were assessed: (1) patient age at the time of final examination; (2) gender; (3) smoking habits; and (4) patient adherence (PA) (i.e., whether a patient came to professional hygiene recall appointments at least every 6 months or at intervals >6 months since placement of the suprastructure).
The following implant site characteristics were considered: (1) the bone graft (i.e., whether the implant was placed in regenerated bone or in pristine bone) and (2) the presence or absence of a membrane covering the graft during the regenerative procedure.
Clinical measurements
The following clinical parameters were assessed at each implant site using a periodontal probe (Williams 14W Probe, Hu-Friedy Mfg. Co., Chicago, IL, USA): (1) the gingival biotype (direct visual assessment, i.e., visibility of the periodontal probe); (2) the presence (≥1 mm) or absence of keratinized tissue (KT) measured as the distance between the peri-implant mucosal margin and the muco-gingival junction at the buccal marginal portion of the implant mucosa; (3) PPD (measured from the mucosal margin to the probeable pocket); (4) BOP; (5) plaque index (PI); and (6) peri-implant recession (REC, defined as the distance between the implant shoulder and mucosal margin). The measurements of PI, BOP, and PPD were performed at six aspects per implant: mesio-buccal, mid-buccal, disto-buccal, and respective lingual/palatal sites. The presence of KT was visually assessed at the mid-facial and mid-oral surfaces. When clinical signs (i.e., BOP with or without suppuration) suggested the presence of peri-implantitis, non-standardized periapical radiographs were taken at the time of the clinical examination with the long cone paralleling technique and film holders (Rinn XCP, Dentsply Corporate, York, PA, USA) and compared with a baseline radiograph taken at the time of prosthesis installation for bone level confirmation [2]. Particularly, the radiographs were scanned to obtain standardized digital images with a resolution of 1,200 dpi. These images were imported and analyzed using specialized computer software (ImageJ v 1.49, Research Services Branch, National Institute of Health, Bethesda, MD, USA). The calibration of the pixel/mm ratio was performed using the length of the implant as a fixed reference point to compensate for potential radiographic distortion. For the assessment of bone loss, the radiographic distance between the implant shoulder level and the most coronal bone-to-implant contact level was measured mesially and distally, parallel with the long axis of the implant. The same blinded examiner performed all radiographic measurements.
Case definition
Implants were considered healthy in case of no BOP or bleeding only at one surface, assuming one point of bleeding as a consequence of trauma from probing, with no suppuration. The presence of peri-implant mucositis was defined by an osseointegrated implant presenting BOP from more than one surface area of the implant [14]. The presence of peri-implantitis was defined as an osseointegrated implant presenting ≥2 mm peri-implant marginal bone loss concomitant with BOP and/or pus on probing from at least one surface area of the implant, associated with PPD ≥4 mm at the time of examination [5]. The measurement of BOP and the presence of suppuration were assessed within 60 seconds of measurements of PPD.
Statistical analysis
Data were collected using Excel (Microsoft, Redmond, WA, USA). Statistical analysis was performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
The statistical evaluation included the Kolmogorov-Smirnov test to evaluate the normality of the distributions. Since the data were not normally distributed, non-parametric tests were used for all comparisons, including the Mann-Whitney U test, the Kruskal-Wallis rank test, or the Pearson χ2 test, as appropriate. To measure the association between the predictor and outcome variable while controlling for confounders, a logistic regression model was used. The data were allowed to enter the model using backward selection with the significance level to remove set at 0.1. Recorded data are presented as mean values, median (interquartile range; IQR) values, or frequencies (%). P-values <0.05 were considered to be statistically significant.
RESULTS
Overall, 62 (60.2%) female patients and 41 (39.8%) male patients aged 26 to 87 years (mean, 60±8.6 years) were randomly enrolled. A total of 421 dental implants were inserted, 244 (58%) into female patients and 116 (42%) into male patients. According to the given definition, out of the 421 implants, 173 (41.1%) presented BOP on more than one surface area of the implant and were therefore considered affected by a peri-implant mucositis. From a deeper analysis by means of periapical X-rays, 19 (4.5%) presented peri-implant marginal bone loss, and therefore the diagnosis of peri-implantitis was made.
The descriptive statistics for the sample are summarized in Table 1. When considering the PPD, the median value (IQR) was 2.6 mm (1.2 mm). Statistically significant differences in probing depths were observed when the measurements were correlated with specific independent variables: age, gender, PA, membrane, bone graft, and REC. Clinically, 248 (58.9%) implants did not present BOP, whereas 173 (41.1%) showed BOP. Differences in BOP were statistically significant when the following independent variables were considered: age, PA, gingival biotype, PI, and REC.
Table 1
The association between the independent variables versus peri-implant probing depth and bleeding on probing

Data are presented as mean, median and interquartile range, or frequencies (%).
PPD, peri-implant probing depth; BOP, bleeding on probing; IQR, interquartile range.
a)Post hoc analysis revealed a statistically significant difference between the older patients (the 65–87 age group) and the other groups (P<0.05).
![]()
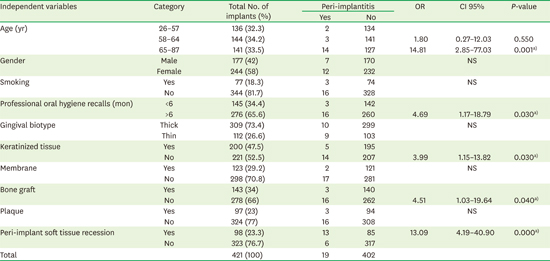
The logistic regression analysis revealed risk factors for peri-implantitis (Table 2). Overall, 5 out of 10 independent variables were significant indicators for peri-implantitis: age (P=0.001), PA (P=0.03), KT (P=0.03), bone graft (P=0.04), and REC (P=0.000). Odds ratio (OR) estimates and 95% confidence intervals (CIs) were retrieved from the intercept of each factor.
Table 2
The risk indicators for peri-implantitis according to the logistic regression analysis
OR, 95% CI, and P-values are reported.
OR, odds ratio; CI, confidence interval; NS, not significant, the independent variable was not a statistically significant predictor of peri-implantitis.
a)Statistically significant difference between the analyzed variables.
![]()
DISCUSSION
The present retrospective study was designed to assess the influence of potential risk factors on the development of peri-implant disease at the implant level. Because multivariate analyses correcting for confounding factors may be indicated in cases of retrospective studies assessing peri-implantitis predictors, a logistic regression model was used. Mean prevalences of peri-implant mucositis and peri-implantitis at 43% and 22%, respectively, have been recently reported [15]. In the present study, prevalences of 41.1% and 4.5% were observed for the peri-implant mucositis and peri-implantitis group, respectively. These results favorably compare with those reported in a recent meta-analysis, in which the frequency of peri-implant mucositis and peri-implantitis were 30.7% and 9.6%, respectively [16]. In the present study, the lower peri-implantitis rate was probably related to the selection of a convenience sample subjected to the same surgical and prosthetic protocol, which may have decreased the prevalence of the event. Moreover, the heterogeneity among studies resulting from differences in case definition and study design may have led to an overestimation of the frequency of the disease.
Because many systemic diseases are chronic and more common in older individuals, and can directly or indirectly compromise implant health, age may be considered a risk indicator. As a confirmation of this hypothesis, the present study indicated that patient age ≥65 years and a low level of patient adherence (>6 months per recall appointment) were strongly associated with peri-implant mucositis (P=0.025 and P=0.046, respectively) and peri-implantitis (OR=14.81; P=0.001 and OR=4.69; P=0.03, respectively). This was also emphasized by the significantly higher PPD values measured in the two groups (2.78 mm; P=0.036 and 2.69 mm; P=0.020, respectively). A similar trend was observed by Ferreira et al. [14] considering a study group of 212 partially edentulous subjects rehabilitated with osseointegrated implants. The authors found slightly higher prevalences of peri-mucositis and peri-implantitis for older individuals (>45 years old) (58.57% vs. 67.60% and 7.14% vs. 9.85%, respectively) and for patients who underwent episodic maintenance visits (>6 months) (61.70% vs. 66.95% and 8.51% vs. 9.32%, respectively). Peri-mucositis showed a correlation with the age of the patients that was also validated by the univariate analysis performed by Roos-Jansaker et al., who found that age (≥60 years old) was a significant risk factor for the development of the disease (P=0.02). This finding is in agreement with a study regarding prevalence and risk variables for peri-implant disease in a comparable cohort sample, which concluded that subjects older than 65 years were more prone to develop peri-implantitis [17]. This may be explained by several factors, namely difficulties in maintaining proper oral hygiene due to impaired vision, lack of dexterity, brain diseases (e.g., Parkinson disease or dementia), and osteoarthritis; increased occurrence of cancer that requires radiotherapy treatment, therefore enhancing the risk of peri-implantitis; lower immunity, compromised healing capacity, and lack of motivation in oral hygiene measures that may arise as a consequence of tooth loss [1819]. Age was also identified as a contributory factor for the development of peri-implantitis when associated with a history of periodontitis and cardiovascular disease [20]. Even the immobility of older patients preventing them from reaching the dental clinic may postpone recall hygiene visits, jeopardizing the efficacy of the implant maintenance program and thus increasing the risk of peri-implant disease. On the other hand, a recent long-term retrospective study evaluating implants placed in subjects older than 65 years found a failure rate of 4.61% at the implant level and 0.02% at the patient level [21]. Thus, it may be suggested that the patient’s age might not represent a factor of major prognostic significance in implant treatment, if meticulous oral hygiene procedures and recall visits are respected. Indeed, inadequate plaque control due to poor accessibility for oral hygiene at implant sites has been associated with peri-implantitis [22].
In the present study, the role of plaque accumulation in terms of increased risk of peri-implant disease led to contradictory results. Despite the failure to demonstrate a clear association between the presence of plaque and peri-implantitis in terms of increased risk of susceptibility, statistically significant differences in terms of a higher percentage of PPD (P=0.005) and BOP (P=0.001) were found. This was probably related to the great heterogeneity within the group with no plaque (n=324) versus the group showing plaque (n=97), which in turn led to misleading results. On the other hand, several studies have pointed out a positive correlation between high plaque scores and increased risk of presenting peri-implant disease [1722]. The primary role of plaque in disease occurrence was also stressed by Ferreira et al. [14], who found a dose-dependent association between higher plaque scores and worse conditions in peri-implants. The OR for plaque score in cases of peri-implantitis (OR=14.3, 95% CI, 9.1–28.7) was much higher when compared with the same level of plaque score in peri-implant mucositis (OR=2.9, 95% CI, 2.0–4.1). In the present study, this was corroborated by the higher likelihood of developing peri-implantitis for patients who underwent professional oral hygiene recall less than twice a year with respect to patients who adhered to the implant maintenance schedule.
Furthermore, the patient's adherence has a consequent effect on the marginal bone levels. Indeed, a lower mean level of bone loss was observed in the adherent group compared with the non-responding group [23]. Hence, the role of supportive maintenance care could be considered a key factor in reducing the risk of implant complications. Accordingly, the absence of preventive maintenance has been associated with significantly worse peri-implant conditions, in terms of PI, BOP, percentage of sites with PD ≥5 mm, number of implants with peri-implantitis, and PBL [24]. Accordingly, data reported in the present study confirmed the fact that the worst PPD and BOP scores were significantly associated with non-adherent patients.
The correlation between peri-implantitis and the presence or absence of KT deserves some discussion. Indeed, the data show a higher incidence of peri-implantitis in patients who did not present KT compared with patients presenting with at least 1 mm of KT (OR=3.99; P=0.03). There has been controversy in the discussion of the impact of KT around dental implants. Soft tissue defects or poor-quality soft tissue at the area of implantation has been considered to be a risk factor for the development of peri-implantitis [25]. This is probably related to the association of a lack of adequate KT around endosseous dental implants with more plaque accumulation, tissue inflammation, mucosal recession, and attachment loss. Conversely, similar studies were not able to find a clear association between the absence of keratinized peri-implant mucosa and peri-implant disease [7826]. The results obtained in the present study corroborated those reported in a recent systematic review, emphasizing the importance of an adequate zone of KT surrounding implants so that better peri-implant tissue health may be achieved [27]. Interestingly, on the other hand, the presence or absence of KT did not influence the likelihood of developing peri-implant mucositis. Thus, one may speculate that implants might be maintained in a healthy condition even in cases of an inadequate width of KT; however, the absence of KT associated with poor oral hygiene is a relevant risk factor for the development of peri-implant disease. This is particularly true when patients without keratinized mucosa are categorized as thin-biotype subjects [28]. Our statistical analyses indicated that a thin biotype was associated with higher percentages of BOP as compared with thick-biotype patients (38.5% vs. 48.2%, respectively). This result can be attributed to thinner tissues being more friable, less vascularized, and accompanied with thinner underlying bone. Furthermore, a thin periodontal biotype is associated with a more shallow biologic width compared with a thick biotype. As a consequence, a thin biotype is more susceptible to biologic width invasion, resulting in marginal tissue recession and alveolar bone loss [29]. This is particularly true in cases of dental implants, due to the fundamental differences that exist between the peri-implant mucosa and its counterpart in natural teeth. Thus, similar to gingival tissue, thin peri-implant soft tissue is more susceptible to soft tissue recession compared with thick peri-implant soft tissue. Therefore, a thin-tissue biotype associated with missing KT is associated with an increased risk of unfavorable treatment outcomes following surgical interventions [30].
This may explain the strong relation between peri-implant soft tissue recession and the occurrence of peri-implantitis. The logistic regression model showed a statistically significant connection between the presence of REC and peri-implant disease (OR=13.09; P=0.00). This might be attributed to the different behavior of the two different biotypes in response to mechanical and/or surgical trauma. Indeed, a thick biotype reacts with the formation of periodontal pockets and intrabony defects, whereas a thin biotype responds with gingival recessions [31]. These results corroborated those of a previous study that reported increased soft and hard tissue resorption to re-establish a healthy peri-implant mucosal dimension, especially in a thin biotype [32]. This explanation favorably compares with a recent observation that the distance between the implant platform level and bone level was greater in individuals with peri-implantitis, indicating that soft tissue recession as a consequence of bone loss negatively influences peri-implant tissue health [20]. A peri-implant soft tissue recession as a consequence of bone loss induced by a peri-implantitis lesion might expose the coronal portion of the implant. Moreover, due to a greater tendency for rougher surfaces to accumulate and retain more plaque, biofilm formation is facilitated [33]. Thus, the relevant correlation between REC and peri-implantitis can also be explained by the fact that, for implants with a coronal roughened surface, such as those evaluated in the present study, a bacterial biofilm forms upon exposure to the oral environment as a consequence of soft tissue recession. Because these microorganisms may persist and proliferate, they are a leading contributor to peri-implantitis, which can lead to the loss of implant integration [34]. Although rough-surface implants are technically more susceptible to bacterial colonization, this has been demonstrated mostly in animal or in vitro studies [3536]. Evidence for the influence of the implant surface characteristics as a risk indicator for peri-implantitis still needs further investigation [37].
The role of the recipient bone (native bone vs. grafted bone) in developing peri-implant disease is still debated. From the data obtained in the present analysis, implants placed in pristine bone had significantly higher PPD (P=0.013) and were more susceptible to develop peri-implantitis (OR=4.51; P=0.04) as compared with implants inserted in regenerated bone. Accordingly, a similar study found that implants in augmented sites have a lower risk of developing peri-implant mucositis when compared with implants placed in non-augmented sites. Regenerating the missing bone provides better hard tissue architecture, allowing for ideal implant placement. As a consequence, the better adaptation of the hard and soft tissue around the implant shoulder might explain a better control against bacterial colonization and greater resistance to bacteria, thus decreasing the probability of developing peri-implantitis [9]. Other studies failed to demonstrate a similar association between augmentation procedures and implant failures [3839]. In contrast, from a different cross-sectional study, the events of peri-implant mucositis and peri-implantitis appeared to be correlated with augmentation procedures. In particular, implants with a fixed prosthesis placed in the upper jaw along with bone augmentation procedures appeared to be more susceptible to peri-implant diseases [8]. Notably, in our department, augmentation procedures are carried out only in non-smoking, healthy patients; this may have had an effect on the outcomes of implant therapy.
Within the limitations of the study, subjects aged 65 years or older and non-adherent subjects were more prone to developing peri-implant mucositis and peri-implantitis to a degree that was statistically significant. At the implant level, the absence of keratinized gingiva, implants placed in pristine bone, and peri-implant soft tissue recessions were statistically correlated with peri-implant disease. Therefore, early diagnosis of peri-implant mucositis associated with the identification of specific risk indicators may prevent subsequent advanced tissue breakdown.
 XML Download
XML Download