

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic periodontitis is a destructive periodontal disease that involves gingival inflammation and bone destruction caused by specific microorganisms, and it is an indication for tooth extraction [123]. Chronic periodontitis is further classified as localized or generalized depending on whether ≤30% or >30% of the sites are involved [4]. The symptoms of chronic periodontitis usually progress without any episode of subjective pain, worsening the periodontal condition [5]. The specific aim of periodontal therapy is to arrest the inflammatory process. Various parameters, including the probing pocket depth (PPD), the clinical attachment level (CAL), tooth mobility, and bleeding on probing (BOP), are routinely used to evaluate the periodontal status. Periodontitis is typically treated by mechanical removal of the supra- and subgingival calculus and improvement of periodontal health through reductions of the PPD, BOP, and tooth mobility and an increase of the CAL [3]. Periodontists must regularly manage periodontitis with a diverse range of disease severity and extent. The available treatments are divided into two types, namely non-surgical and surgical therapies. Additionally, adjunctive treatments (antimicrobials or laser therapy) are also available [6789]. The American Academy of Periodontology (AAP) suggests that the most minimally invasive and cost effective periodontal treatment should be adopted, and this is usually performed through non-surgical treatments, such as scaling and root planing (SRP). Furthermore, the American Dental Association Council on Scientific Affairs presented an evidence-based clinical practice guideline on the non-surgical treatment of patients with chronic periodontitis by means of SRP with or without adjuncts [89]. They evaluated four adjunctive therapies such as systemic subantimicrobial-dose doxycycline, systemic antimicrobials, chlorhexidine chips, and photodynamic therapy with a diode laser, which are beneficial in the non-surgical treatment of chronic periodontitis with a moderate level of certainty [9]. However, when the periodontal condition does not recover with a non-surgical treatment, surgical treatment is considered to restore periodontal health.
In the periodontally compromised tooth, the normal occlusal force could affect the periodontal tissue and cause further attachment loss [10]. First, the signs of inflammation must be resolved. When the periodontal condition becomes stable, occlusal adjustment can be considered [11]. Trauma from occlusion (TFO) refers to an injury to the periodontal attachment components caused by abnormal occlusal force. TFO is divided into three categories: primary, secondary, and combined occlusal trauma [12]. Primary occlusal trauma results from excessive occlusal force with normal periodontal support. On the other hand, secondary occlusal trauma is caused by excessive or premature contact on teeth with a damaged periodontium. Many animal experiments and clinical studies have investigated the role of occlusion in the pathogenesis of periodontitis [1213141516]. The results suggest that premature contact or excessive occlusal force could be an etiologic factor in the progression of periodontitis through inflammation that spreads into the deep portion of the periodontium. Based on these findings, vertical alveolar bone resorption and infrabony defects should be considered a result of occlusal trauma [1718]. Here, we describe a successful non-surgical treatment with adjunct therapy in a periodontally compromised tooth with a secondary TFO showing alveolar bone regeneration. The use of the patient records was approved by the Institutional Review Board (ERI15007) of Seoul National University Dental Hospital (SNUDH).
CASE DESCRIPTION
Patient information and diagnosis
A 38-year-old man with a non-contributory medical history presented at the Department of Periodontology, SNUDH, Seoul, Korea, with a chief complaint of continuous buccal sinus tract formation of the maxillary left 1st premolar (#24). A clinical examination revealed a sinus tract with pus discharge at the buccal surface and hyper-tooth mobility, and Angle class III malocclusion and anterior cross-bite were observed. In the periapical radiograph, extensive radiolucency and active bone resorption around the root were noteworthy, and subgingival calculus deposition was observed (Figure 1A). The PPD was approximately 9–10 mm at the distal portion and 7–8 mm at the mesial portion of the #24 tooth. The diagnosis was localized chronic periodontitis with secondary TFO. Because of a periapical lesion, endodontic treatment was also considered. However, the tooth was responsive to the electric pulp tester (EPT), and periodontal treatment and occlusal adjustment were planned first.
Figure 1
Periapical radiography: (A) Initial radiography showing a periapical radiolucency and severe bone resorption of the maxillary left first premolar, which has subgingival calculus deposition. (B-F) Follow-up, 3 (B), 6 (C), 9 (D), 12 (E), and 16 months (F) after periodontal treatment and occlusal adjustment.

Treatment
Subgingival calculus was removed by root planning, and inflamed soft tissue was managed by subgingival curettage. Minocycline ointment was locally applied to the deep gingival pocket, and antibiotics (100 mg cefdinir 3 times daily) and anti-inflammatory analgesics (650 mg acetaminophen 3 times daily) were prescribed for 5 days. At the next visit 2 weeks later, the patient reported that the gingival condition was more comfortable than before the treatment. The gingival inflammation was dramatically reduced and showed no sinus tract or pus discharge upon oral examination. However, the tooth mobility was still severe, and occlusal interference during canine guidance and premature occlusal contact were observed. Tooth splinting with a dead soft wire and composite resin on the palatal side and occlusal adjustment were performed. The premature contact was marked as the ‘high spot’ with a check bite (AccuFilm II, Parkell, Edgewood, NY, USA), and it was simply removed with selective grinding. After tooth splinting and occlusal equilibration, root planing was performed once more, and antibiotics (500 mg amoxicillin, 3 times daily) and anti-inflammatory analgesics (100 mg aceclofenac, 2 times daily) were prescribed for 5 days. At a re-check after 2 weeks, the PPD was slightly reduced and the inflammatory signs were nearly resolved.
Follow-up and results
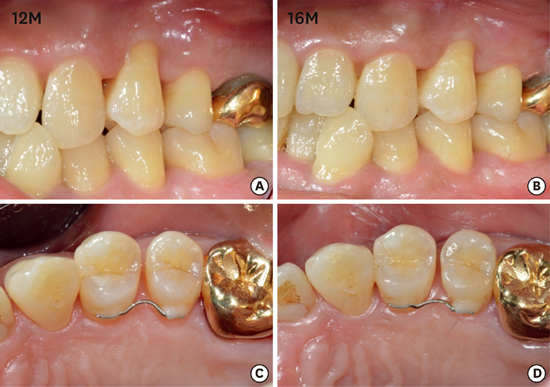
The patient was recalled periodically (3, 6, 9, 12, 16 months), and a follow-up radiographic examination showed noteworthy improvement of the periapical radiolucency (Figure 1B-F). Interestingly, alveolar bone regeneration was observed and maintained, showing new periodontal ligament attachment at the root surfaces including the surrounding teeth, as indicated with arrows in Fig. 1F. The clinical examinations included a pulp vitality test with an EPT, recordings of the PPD, tooth mobility, and a percussion test performed 16 months after treatment (Table 1). The tooth (#24) vitality was maintained, PPD was recovered within a normal range around 3–4 mm, and there was no symptom in the percussion test. As wire was attached at both sides of the #24 tooth, a proper tooth mobility check was not performed until the 12-month examination. The wire that was attached to the tooth with a composite resin was partly detached after 12 months of follow-up, and the mobility was examined. Tooth mobility was dramatically reduced, and it was assumed that this was the result of alveolar bone regeneration (arrow, Figure 1F). The gingival condition was well maintained without any signs of inflammation (Figure 2); however, buccal gingival recession was observed (Figure 2).







DISCUSSION
The relationship between periodontal condition and occlusal trauma has been discussed for a long time [19]. A healthy periodontal condition endures occlusal force and inhibits periodontal pocket formation; otherwise, periodontitis combined with occlusal trauma leads to periodontal destruction or vice versa [20]. In the presented case, subgingival calculus deposition was observed; however, this might not be a critical factor involved in the severe periodontium destruction surrounding tooth #24, considering the generalized subgingival calculus deposition. Instead, inappropriate canine guidance by the anterior crossbite and Angle class III malocclusion might be critical factors in the destruction of the periodontium. The lack of canine guidance induces contact with the molars in ways that generate sideways forces. These unfavorable forces can cause tooth mobility, possibly accompanied by alveolar bone resorption, progressing to tooth extraction. In the case of secondary TFO, including the degraded periodontium, occlusal adjustment/tooth splinting and periodontal treatment are necessary to eliminate the occlusal trauma caused by occlusal interference.
In the present case, the periodontal condition was diagnosed with a panoramic view in the first oral examination. Usually, in the panoramic view, the condition of tooth #24 is not remarkable, and distinguishing the apical radiolucency is difficult because of superimposition with other anatomical structures, as in this case (Figure 3). In the oral examination of a patient, radiographic examination is a critical aspect of diagnosis, and currently digital panoramic radiography is widely used due to its convenience and ability to achieve broad coverage of the alveolar bones and teeth [21]. Despite the many advantages of the panoramic view, anatomical overlap or image distortion might miss important features such as periapical pathology, bone resorption, and caries [22]. In this case, the exact diagnosis of the periodontal condition of the teeth was difficult using the panoramic view; on the other hand, the periapical view offered more detail with a focus on the specific teeth. Therefore, periapical radiography is essential for the proper diagnosis of the periodontal condition and evaluation of the patient’s records.

In every practice, dentists are faced with the decision of whether or not to save a tooth. Although the maintenance of natural teeth has been accepted as a primary goal of dentistry, with the remarkable development of dental implant systems, tooth extraction and implant placement have become an easy treatment option in patients with periodontally compromised teeth. On the other hand, there is a risk of overuse of this approach without an effort to conserve the natural dentition. Therefore, a prudent approach to ensure accurate diagnosis and treatment planning is needed before finalizing the decision for extraction.
 XML Download
XML Download