

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic periodontitis is an inflammatory disease that induces gingival recession, loss of the periodontal ligament, and destruction of the alveolar bone after periodontal pocket formation caused by pathogenic microbial plaque [1]. As periodontal destruction progresses in an apical direction, the furcation can become exposed in molar teeth. Failure to institute proper periodontal treatment might result in loss of the tooth.
In order to prevent progression, it is important to determine the etiologic factors in periodontal disease. Attar and Phadnaik [2] suggested four local factors that can contribute to inflammatory and degenerative periodontal disease: (1) conditions that propagate plaque retention and accumulation, (2) abnormal anatomical tooth structures, (3) habits and self-inflicted injuries, and (4) mechanical factors such as improper tooth brushing and the use of abrasive dentifrices and other oral hygiene modalities (e.g., dental floss and oral lavage). Several developmental variations in tooth morphology such as palatogingival grooves, cervical enamel projections (CEPs), and enamel pearls can induce the accumulation of plaque. The nature and location of such features may also compromise effective removal of plaque by both patients and health professionals [3].
CEPs have been defined as the extension of enamel beyond the cementoenamel junction in an apical direction toward the furcation area of molars [45]. Since an association between enamel projections and periodontal pockets was first noted by Atkinson [6] in 1949, these projections have received attention as a cause of localized periodontal tissue destruction [78]. Several studies have shown a positive correlation between the prevalence of CEPs and furcation defects [91011]. Masters and Hoskins [4] suggested that in areas where the enamel extends into the root furcation, the fibers of the periodontal ligament are not truly attached to the tooth. Machtei et al. [12] reported that periodontal pockets were deeper in teeth that showed enamel projections than in teeth without CEPs in patients who had Class II furcation defects. Because of their incomplete union with the periodontal attachment apparatus, some have recommended that enamel projections be removed [2711]. However, during periodontal surgery, especially in patients with grade III CEPs, it is almost impossible to determine whether the enamel projections have been completely removed in vivo. Therefore, we sought to determine how effective conventional rotary instruments are in removing enamel projections, and to compare the characteristics of tooth surfaces treated with each of three different instruments. To do so, we conducted in vitro experiments using extracted human molars.
MATERIALS AND METHODS
Selection and preparation of teeth
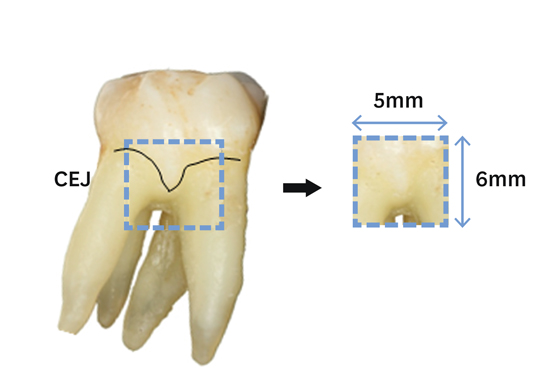
We selected 60 extracted molars from patients who had a history of periodontal disease but who had not undergone restorative treatment for cervical abrasion. All the teeth clearly showed CEPs, which were designated grade I, II, or III according to Masters and Hoskins’ classification criteria [4] (Table 1), with 20 teeth in each group. A Gracey curette 11/12 (Hu-Friedy, Chicago, IL, USA) was used to remove any soft tissue and calculus still attached to the root surfaces. By embedding each tooth in gypsum, with the furcation area exposed, we created conditions similar to those in the mouth (Figure 1).
Table 1
Classification of cervical enamel projections (CEP) [4]


The CEPs in each group were removed with three different rotary instruments: (1) a piezoelectric ultrasonic scaler (P-MAX) (Satelec-Acteon, Seoul, Korea) with an H4R tip; (2) a 368 014 5ML periodontal bur ("Paro" Periodontology Kit, Diatech, Rolle, Switzerland) used in a handpiece at low speed (<25,000 rpm); and (3) a thin, tapered SF104R diamond bur (Shofu, Kyoto, Japan) used in a handpiece at high speed along with water irrigation (Figure 2). Abrasion was carried out carefully, with the tooth surface being repeatedly dried with compressed air to detect any remaining enamel, until the projections had been completely removed, as judged with the naked eye.

Preparation of specimens
After the CEPs were removed, we prepared final specimens that contained the cementoenamel junction, 5×6×2 mm3 in size, with a high speed bur, (Figure 3). We did not use any solution or agent for clearly detecting and comparing the roughness or the remnants of the enamel, in order to perform further cell attachment experimentation using these tooth specimens.
Evaluation of root surface characteristics using scanning electron microscopy (SEM)
Tooth specimens were coated with gold particles and examined using SEM (FE-SEM S-800) (Hitachi, Tokyo, Japan) before and after CEP removal. We analyzed the characteristics of the tooth surfaces with respect to roughness and whether the projections had been completely removed at magnifications of 20×, 100×, 200×, and 1,000×. The tooth surfaces were instrumented and analyzed by one person who was well trained in periodontal treatment.
RESULTS
Representative SEM images of CEPs in either grade I or grade II are shown in Figures 4, 6, and 8, because the surface characteristics after removal of the enamel projections were similar for these two groups. Representative images of CEPs in grade III are shown in Figures 5, 7, and 9.
Figure 4
Representative SEM photographs of tooth surface before (A) and after (B and C) removal of grade II cervical enamel projections with the use of an ultrasonic scaler (A, B: 20×, C: 200×).

Figure 6
Representative SEM photographs of tooth surface before (A) and after (B and C) removal of grade I cervical enamel projections with the use of a periodontal bur (A, B: 20×, C: 200×).

Figure 8
Representative SEM photographs of tooth surface before (A) and after (B and C) removal of grade II cervical enamel projections with the use of a diamond bur (A, B: 20×, C: 200×).

Figure 5
Representative SEM photographs of tooth surface before (A) and after (B and C) removal of grade III cervical enamel projections with the use of an ultrasonic scaler (A, B: 20×, C: 200×).

Figure 7
Representative SEM photographs of tooth surface before (A) and after (B and C) removal of grade III cervical enamel projections with the use of a periodontal bur (A, B: 20×, C: 200×).

Figure 9
Representative SEM photographs of tooth surface before (A) and after (B and C) removal of grade III cervical enamel projections with the use of a diamond bur (A, B: 20×, C: 200×).

Surface characteristics after removing CEPs with an ultrasonic scaler
The ultrasonic scaler failed to completely remove CEPs of all three grades (I, II, and III), as evident with SEM (Figure 4B and 5B). The presence of enamel remnants was clearer at higher magnification, and the tooth surface was rough at the periphery of areas where CEPs had been removed (Figure 4C and 5C).
Surface characteristics after removing CEPs with a periodontal bur
When the periodontal bur was used to remove the enamel projections, the outlines of the CEPs of all three grades seemed to disappear completely at low magnification (20×) (Figure 6B and 7B). However, enamel remnants could be seen at higher magnification (200×) (Figure 6C and 7C). The tooth surfaces were generally smoother than those attained with the ultrasonic scaler, although a corrugated rough surface appeared at regular intervals corresponding to the size of the bur (Figure 7C). Removal of cementum adjacent to enamel projections was confined to the outer layer of the tooth surface, indicating that the periodontal bur was not invasive.
Surface characteristics after removing CEPs with a diamond bur
Grade I, II, and III CEPs disappeared completely with abrasion by the diamond bur, and the smooth surface showed a combed pattern at regular intervals corresponding to the size of the bur. At 200× magnification, the surfaces treated with the diamond bur were smoother than those treated with the ultrasonic scaler and the periodontal bur (Figure 8 and 9). The diamond bur produced multiple layers on the root surface and was invasive, especially for the grade III CEPs, whereas the periodontal bur produced a uniform and shallow surface (Figure 7C, 8C, and 9C).
Exposure of dentinal tubules after CEP removal
After the enamel projections were removed, specimens were randomly selected for examination at a much higher magnification (2,000×) to determine whether or not dentinal tubules had been exposed (Figure 10). Most of the specimens treated with the ultrasonic scaler did not show dentinal tubules, because this instrument failed to remove the enamel projections completely. Although the entrances of the dentinal tubules were detected in most of the specimens treated with the periodontal bur and the diamond bur, they were occluded by a smear layer.

DISCUSSION
Periodontal disease is caused by bacterial plaque, and developmental tooth deformities can provide good hiding places for the accumulation and retention of plaque [1314]. Localized periodontal bone destruction occurs in areas with chronic plaque accumulation and developmental abnormalities. In particular, the cervical part of the tooth seems to be sensitive to local irritation by external factors. Masters and Hoskins [4] were the first to name and classify the extensions of enamel that protrude into the furcation as “cervical enamel projections” and reported their incidence as 17% in the maxilla and 29% in the mandible. They also noted that almost 90% of the teeth in which enamel involved the furcation showed these projections [4]. Grewe et al. [7] reported that the grade I CEP is most common, followed by grade III, with incidences of enamel projections of 8.2% in the maxillary first molar and 35.5% in the mandibular second molar. Cho and Choi [15] reported that the incidence of CEP was 73.1% in Korean patients with chronic periodontitis. The incidence of enamel projections in both maxillary and mandibular molars was much higher on the buccal aspects, and grade III CEPs were the most common in their study.
Histological studies of enamel projections have rarely been performed. It has been reported that grade III CEPs are commonly covered by cementum within the confines of the furcation and a capsule-like structure with irregular cementum [816]. We also found irregular, cementum-like globular bodies similar to those reported by Moskow [16] in several SEM specimens. The clinical significance of these bodies has yet to be determined.
Grewe et al. [7] and Bissada and Abdelmalek [17] suggested that there was a strong association between enamel projections and furcation defects. Attar and Phadnaik [2] argued that the enamel projections should be removed to facilitate periodontal maintenance. Based on previous studies, enamel projections have usually been removed in the clinical setting with the use of several types of rotary instruments. However, it remains to be determined which rotary instrument would most effectively remove CEPs and give the result of a hard, smooth surface that would be biocompatible with periodontal ligament cells. Therefore, we performed this in vitro study to investigate and compare the surface characteristics after CEPs were removed using three different rotary instruments.
One of the practical goals of root planing is to achieve the smoothest root surface possible [18]. Therefore, we wished to investigate the results of CEP removal by rotary instrumentation by evaluating surface smoothness and evidence of enamel remnants. Although several experimental studies have reported that roughness of the root surface does not affect the recovery of periodontal tissue [1920], we assumed that it might accelerate the accumulation of bacteria and calculus [182122]. Although researchers have compared the roughness of the root surface after planing with several different rotary and hand instruments [232425], almost no studies have examined the root surface after CEPs have been removed.
SEM images showed that the diamond bur was the most effective instrument in removing CEPs, followed by the periodontal bur and then by the ultrasonic scaler. The diamond bur produced the smoothest surface, whereas the piezoelectric ultrasonic scaler left a very rough surface. These findings are in general agreement with that of previous reports [26].
There were no differences among the CEP grades with respect to removal capacity, although the diamond bur proved to be more invasive to the adjacent tooth surface than the other two instruments after the removal of grade III enamel projections. We assumed that a thin, tapered SF104R diamond bur is bigger than the width of the furcation entrance, which has an average diameter of 1 mm or less; in one report, the diameter of the furcation entrance was 0.75 mm or less in 58% of cases [27]. The ultrasonic scaler caused relatively little damage to the tooth surface because it had a specifically designed tip. Although the periodontal bur left remnant enamel in some specimens, it was able to produce a smooth root surface, meaning it would allow stable attachment of gingival tissue. Because the cementum around the enamel projections was minimally damaged and only superficially removed by the periodontal bur, as opposed to the diamond bur, the periodontal bur appears to be a safer choice for removing class III CEPs in the clinical setting.
In teeth treated with the periodontal bur and the diamond bur, the entrance to dentinal tubules was identified on SEM at high magnification (2,000×), but direct exposure of the entrances was not observed, because they were occluded by a smear layer. Therefore, we inferred that the occurrence and persistence of dentin hypersensitivity were less likely after CEP removal.
This study had some limitations, in that it was difficult to determine precisely how far the grade III CEPs extended into the furcation roof. Therefore, new methods for preparing specimens that involve the entire furcation roof area should be explored in future studies. More precise information about the history of periodontal treatment will become available as we collect and study extracted teeth, allowing us to detect and compare surface changes more accurately. Based on a report by Blanchard et al. [8] that the apical part of enamel projections was covered with cementum, cutting instruments that improve the recovery of periodontal tissue can be identified if the cell adhesion and proliferation test using periodontal ligament fibroblasts and gingival fibroblasts is performed on root surfaces from which CEPs have been removed.
In conclusion, this study examined the root surface of extracted teeth both before and after the removal of enamel projections. In SEM photographs, the diamond bur produced the smoothest surface but was very harmful to the tooth structure near the CEPs. The piezoelectric ultrasonic scaler produced the roughest surface but was less harmful to the tooth structure near the furcation entrance. Further studies will be needed to find the most bioacceptable method for removing enamel projections, including in vitro experiments on periodontal ligament cell attachment and clinical studies on dentin hypersensitivity after CEP removal.
 XML Download
XML Download