

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dental implants have become a highly successful and routine treatment option for the replacement of lost teeth, with a survival rate of more than 89% reported during 10-15 years of follow up [123]. However, the prevalence of peri-implant diseases can limit clinical success and impose health and financial burdens to patients and health providers [45]. Peri-implant diseases following successful integration of an endosseous implant are reported to be the result of an imbalance between bacterial load and host defense [67]. Bacterial accumulation initiates the inflammatory response of soft tissue around dental implants similar to periodontal tissue [89]. Peri-implant diseases may affect the peri-implant mucosa only (peri-implant mucositis) or also involve the supporting bone (peri-implantitis) [10]. The prevalence of peri-implant mucositis has been reported in the range of 39.4-80%, while the frequency of peri-implantitis has been reported to occur in 11.3-47.1% of cases [1112131415]. Diagnosis of peri-implantitis is including the marginal bone loss around implants in radiography with clinical examination of increase of pocket depth, presence of bleeding on probing and suppuration [716].
If peri-implant infection is diagnosed, there are many therapeutic options to avoid implant removal [17]. To limit the progression of the disease, physical removal of the bacterial plaque biofilms is essential either through a non-surgical method or a surgical method [1819]. Lang et al. [192021] suggested a sequential and cumulative fashion, referred to as the cumulative interceptive supportive therapy (CIST) protocol for peri-implantitis treatment: (1) mechanical debridement to remove the biofilm from the implant; (2) antiseptic treatment to decontaminate the implant surface; (3) antibiotic treatment to eliminate infectious bacteria in the surrounding peri-implant tissues; and (4) resective surgery/regeneration to reestablish the bone-implant interface (i.e., re-osseointegration). Only when peri-implantitis causes complete loss of osseointegration, resulting in mobility of the implant, is extraction indicated.
However, the design of the suprastructure may hinder measurements of the probing pocket depth of the infected implants at regular maintenance and cause delay in peri-implantitis diagnosis. If undiagnosed, peri-implant disease may lead to complete loss of osseointegration and eventual implant loss. Hence, regular radiographical check-up for marginal bone loss has been emphasized for early detection of peri-implantitis [2223]. Early peri-implantitis diagnosis is followed by early intervention surgically or non-surgically, which may be beneficial for maintaining marginal bone level after peri-implantitis diagnosis. According to Charalampakis et al.'s study [24], early development of peri-implantitis was significantly associated with implant failure. Consequently, early detection of peri-implantitis and following interventions for peri-implantitis treatment is critical for the survival of peri-implantitis involved implants. However, there have been exceptionally few studies on the relationship between timing of peri-implantitis diagnosis (time required for diagnosis as peri-implantitis after completion of prosthetic procedures) and prognosis of peri-implantitis treatment. Therefore, this study aimed to reveal that early detection of disease could be beneficial on the preservation of marginal bone after peri-implantitis diagnosis.
In this study, the effect of timing of peri-implantitis diagnosis was investigated in patients who had been non-surgically treated and regularly visited for follow-up examinations for more than 5 years. The aim of this study was to determine whether early diagnosis and non-surgical treatment can result in a favorable outcome in maintaining a marginal bone level.
MATERIALS AND METHODS
Patients
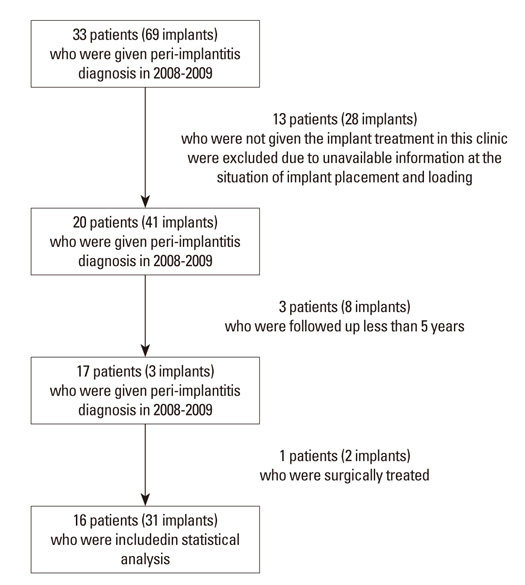
In this study, 33 patients (69 implants) who had been given diagnoses as peri-implantitis from 2008 to 2009 at the Department of Dentistry in Seoul National University Bundang Hospital were included. This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No: B-1111-139-107).
Peri-implantitis was diagnosed by both clinical and radiographic examinations such as the presence of plaque, the presence of bleeding on probing, suppuration, more than 4 mm of probing pocket depth, and more than 2 mm bone loss on radiologic evaluation [16]. After peri-implantitis was diagnosed, patients had a non-surgically or surgically treatment according to CIST protocol (Supplementary Table 1). Non-surgical treatment was mainly performed as follows; curettage of granulation tissues, laser detoxification (Er-YAG laser therapy coding as peri-implantitis treatment: tip; 2061-cylinder, Energy;100 mJ, frequency; 10Hz, Irrigation on, Manufactured by K.e.y Laser®, KaVo, Biberach, Germany), chlorhexidine irrigation, and minocycline ointment injection. Surgical debridement with flap elevation was performed as surgical treatment. At the recurrence of inflammatory symptom such as bleeding on probing and pus discharge with pocket depth >4 mm, re-treatment was performed (1-8 times during the observation period). Regular plaque control and oral health education were performed regardless of non-surgical and surgical treatment of peri-implantitis. Professional tooth cleaning procedures were performed at the regular recall-check by dental hygienist.
A retrospective review of all 69 cases was accomplished using the dental charts and radiographs. Data were collected on diagnosis of chronic periodontitis [25], periodontal treatment before or after implant placement, location of implants, date of implant placement, implant type (external or internal type), implant diameter, lengths, bone regeneration procedures, bone graft materials and barrier membrane used in bone regeneration procedures, exposure of implant thread at the implant placement, residual bone heights at the sinus window procedures, date of loading, type of prosthesis (splinted or single), probing pocket depths at diagnosis of peri-implantitis, and treatment modalities after peri-implantitis diagnosis and during follow-up periods. In regard to the medical condition, medical records from this hospital were reviewed. For cardiovascular disease (CVD), a history of disease was assigned, regardless of disease severity and included angina, stroke, ischemia and high blood pressure with medication [26].
For statistical analysis, 13 patients (23 implants) among 33 patients (69 implants) were excluded due to their missing data (Fig. 1). Since they had given implant treatment in other clinic, we could not access their radiographs and records before peri-implantitis diagnosis. Additionally, 8 patients with 10 implants were excluded because of their follow-up periods with less than 5 years after peri-implantitis diagnosis. At last, only non-surgically treated and more than 5 years followed-up implants (16 patients, 31 implants) were included in statistical analysis, excluding one patient with surgically treated two implants.
Radiographic analysis
A radiographic examination was conducted by one examiner (Park SY), who did not participate in any treatment intervention including implant placement, peri-implantitis treatment and regular recall check. Intraclass correlation coefficient was 0.89 assessing three measurements before and after examination. When comparing the marginal bone height, the junction of the abutment and implant fixture in the radiograph was used as the primary reference point. Radiographs were taken with the parallel technique (Heliodent DS; Sirona Dental Systems, Bensheim, Germany/ Schick Sensor, Schick Technologies, Long Island City, NY, USA) by a trained radiologist. The distance between the implant-abutment junction on the mesial and distal side of the implant and the top of the alveolar crest in periapical radiographs were measured. The values of periapical radiographic images were saved in DICOM format (Digital Imaging and Communications in Medicine, PACS view) calculated as a mean value (Fig. 2). Initial bone level (2 weeks recall-check for re-tightening after final prosthesis delivery; A), diagnosis of peri-implantitis (B), and 5 years after peri-implantitis diagnosis (C) were measured (Fig. 3). For measurement of marginal bone level at loading, periapical radiographs taken at a check-up visit for re-tightening after final prosthesis delivery were applied.
Statistical analysis
Statistical analysis was performed using commercially available softwares (PASW Statics 18.0, SPSS Inc., Chicago, IL, USA;STATA/SE13, Stata Corp, College Station, Texas, USA). To test the normality of data, Kolmogorov-Smirnova test was performed. To compare bone levels at each interval, paired t-test was done. To examine which variables affected the marginal bone level at each interval, Student's t-test or one-way ANOVA was performed. To assess the variables affecting bone loss between each interval, univariable linear regression analysis was performed. Using variables significantly affecting marginal bone level and bone loss at each interval with P<0.05, mixed effect regression model was constructed. A P-value of <0.05 was considered to indicate a statistically significant difference.
RESULTS
In total, 31 implants from 16 patients were included (Tables 1 and 2, Fig. 4). Among 31 implants with peri-implantitis, 29 implants had a bone graft procedures at the implant placement; 6 implants of 29 implants had simultaneous bone graft procedures through lateral sinus window. A probing pocket depth of 6.19±2.75 mm was recorded and a 4.21±2.26 mm of marginal bone level from fixture-abutment connection was observed at peri-implantitis diagnosis. Marginal bone change at each interval was shown in Table 3. The total survival period of all implants after loading was an average of 79.23±19.47 months (survival periods after implant placement: 85.48±19.05 months). Three out of 31 implants were removed from the jaw during follow-up periods. One implant of molar region in maxilla was failed at 59 months after peri-implantitis treatment. The other two implants were strategically removed for additional prosthetic procedures of adjacent missing teeth.
Factors affecting marginal bone levels at each interval
Marginal bone levels at each interval according to the variables were shown in Table 4. Implants in male patients were significantly deeper marginal bone level than those in female patients at each interval (Table 4). In addition, patients with CVD and CM showed more significantly deeper marginal bone levels at each interval than healthy patients and patients with CVD. Among 31 implants, 24 implants were placed in patients who had a diagnosis of periodontitis, which did not significantly influence marginal bone levels at each interval. Instead, patients who are needed to be periodontally treated before implant placement showed significantly deeper marginal bone levels at each interval than those who were periodontally treated after implant placement.
In maxillary molar region, more significantly deeper bone levels at each interval were shown than mandibular molars and it was significant. Implant diameters and lengths did not significantly affect marginal bone levels. During bone grafting procedures, use of membrane and thread exposure at implant placement significantly influenced the marginal bone levels. Most of implants were splinted and it did not influence the marginal bone levels.
Mixed-effect regression analysis
To investigate the effects of variables on marginal bone loss, multivariable analysis was constructed using variables with factors affecting marginal bone level (Table 4) and bone loss between each interval (Supplementary Table 2). As a result, mixed model regression analysis was performed at fixed variables of timing of peri-implantitis diagnosis, bone level at loading, gender, systemic disease, periodontal status, location of implants, and surgical factors and random variables of patients. To avoid collinearity, bone level at peri-implantitis diagnosis was not included in this model (correlation r=0.789, P<0.001 between timing of peri-implantitis diagnosis and bone level at peri-implantitis diagnosis).
Timing of peri-implantitis was one of the significant factors affecting initial bone loss and total bone loss not additional bone after peri-implantitis diagnosis (Table 5). Patients with CVD and DM were positively influenced on both initial bone loss and total bone loss. Patients who needed periodontal treatment after implant placement showed a negative effect on bone loss compared to those who needed periodontal treatment before implant placement during entire periods. Implant location also significantly influenced on amounts of bone loss. Mandibular implants showed less bone loss than maxillary implants. Among surgical factors, combined use of autogenous and xenogenic bone graft materials showed a negative effect on bone loss compared to autogenous bone graft materials. Use of membrane negatively affected on initial bone loss but positively on additional bone loss and total bone loss. Thread exposure showed positive effects on initial bone loss and total bone loss.
DISCUSSION
We set out to determine whether early diagnosis of peri-implantitis might be of benefit in minimizing bone loss through non-surgical treatment and whether it would be possible to clarify the potential role of regular check-ups after diagnosis of peri-implantitis. In peri-implantitis treatment, early diagnosis of peri-implantitis has been emphasized but its impact on the marginal bone loss was not fully investigated. This retrospective study evaluated the effect of timing of peri-implantitis diagnosis on the change of marginal bone loss following non-surgical peri-implantitis for more than 5 years. As a result, earlier peri-implantitis was advantageous in preservation of marginal bone level after peri-implantitis treatment.
In this study, marginal bone levels during entire treatment periods were significantly affected by systemic disease of patients and periodontal inflammations. Renvert et al. [26] also demonstrated a significant relation between peri-implantitis and CVD, and reported an odds ratio of having peri-implantitis and a history of CVD of 8.7. However, CVD alone in this study did not cause harmful effects on peri-implant disease whereas CVD with diabetes did significantly affect the marginal bone level. However, amount of the additional bone loss after peri-implantitis diagnosis was not significantly different regardless of systemic diseases and periodontal status, which may be related to early detection of peri-implantitis and regular check-up after peri-implantitis diagnosis. Therefore, patients in high risky group could also use the dental implants without complication related to peri-implantitis if they are regularly checked up and professionally cleaned after implant placement.
In this study, the amount of initial bone loss significantly correlated to timing of peri-implantitis. Schwarz et al. [27] stated that non-surgical treatment is recommended for marginal bone loss less than 2 mm around implant and surgical treatment such as apically positioned flap or flap surgery is recommended for marginal bone loss greater than 2 mm. Therefore, earlier detection of the disease may result in less invasive treatment modality for peri-implantitis treatment. In the current study, majority of cases were diagnosed as peri-implantitis less than 4 years after loading. They showed about 2 mm of marginal bone loss and were non-surgically treated. Although non-surgical treatment combined with laser application achieved favorable clinical results, non-surgical treatment is difficult to promote re-osseointegration and additional surgical approaches are needed to minimize reinfection of the periodontal pocket around the implant. Consequently, early detection of peri-implantitis may be helpful for minimizing the patient's discomforts and costs related to surgical intervention.
For earlier detection of radiographic change of implants, regular check-up is necessary for the patients with the risks of peri-implantitis. Although some patients did not follow the regular check-up program before peri-implantitis diagnosis, all patients regularly visited after peri-implantitis diagnosis and were taken professional cleaning procedures at 3-5 months intervals during more than 5 years. As a result, the bone level of non-surgically treated 31 implants was well-maintained more than 5 years follow-up periods. Additional bone loss after non-surgical therapy was approximately 0.5mm in average during follow-up periods although the recurrence of inflammation appeared in some cases during follow-up periods and repetitive non-surgical therapy was performed to resolve the inflammation. The importance of regular supportive care to maintain the periodontal and peri-implant health has been emphasized in previous studies [2829]. Recently, Lagervall and Jansson [30] reported that the success rate of peri-implantitis treatment was significantly lower in the patients with poor oral hygiene and low compliance regardless of their treatment modalities. Similarly, Serino and Ström [31] presented the importance of proper oral hygiene instructions in maintaining of healthy peri-implant tissue.
Most of implants in this study underwent bone regenerative procedures including lateral sinus lift. Thread exposure at implant placement and use of barrier membrane and graft materials during regenerative procedures affected bone levels at each interval. They also influenced amounts of bone loss between each interval. Although use of membrane reduced initial bone loss, it increased additional bone loss after peri-implantitis diagnosis. Thread exposure at implant placement was also one of the important factors affecting initial bone loss. Xenograft alone showed a positive effect on initial bone loss and total bone loss compared to autogenous bone graft. However, combined use of autogenous and xenogenic showed negative effects on bone loss during entire periods compared to autogenous bone alone group. Therefore, to prevent development of peri-implantitis, sites of implant placement should be considerately determined from the initial step of treatment planning, which is followed by careful surgical procedures to avoid the implant thread exposure. When implant threads are exposed, use of barrier membrane and combined use of autogenous bone and xenogenic graft materials may be advantageous in preservation of marginal bone level.
One of the limitations of our study is related to its small sample size and retrospective nature. For analysis of relationship between marginal bone loss and timing of peri-implantitis diagnosis, this study included only cases in which the entire implant treatments, procedures including implant placement, peri-implantitis treatment and follow-up were conducted in our own clinic. In addition, this study included only patients who followed-up more than 5 years after peri-implantitis diagnosis. Waerhaug [32] previously suggested that the evaluation of treatment outcome can only be safely conducted after about 5 years in cases with deep pockets. Accordingly, the mean follow-up period was relatively more homogeneous than other survival studies and confounding factors affecting multivariate regression analysis such as marginal bone level change at the time could be minimized. Additionally, we attempted to adjust the effect of multiple implants in the same patients through a mixed-effect regression model analysis. Therefore, despite its small sample size, these results may be meaningful in decision-making for peri-implantitis treatment modalities. To confirm this study, well-designed clinical trials and experimentally controlled investigations are needed in further studies.
In conclusion, early diagnosis of peri-implantitis can be beneficial in minimizing initial bone loss, leading minimal amounts of total bone loss. This favorable result was obtained from non-surgical treatment owing to their small amount of bone loss at diagnosis of peri-implantitis. Additionally, this study may also provide the evidence about regular check-up after implant treatments.









 XML Download
XML Download