

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Peri-implant mucositis is defined as inflammation in the mucosa around a dental implant. Gingivitis and peri-implant mucositis are similar in that both are reversible [1]. Early intervention with effective removal of the microbial biofilm is known to be helpful in preventing further progression to periodontitis and peri-implantitis, respectively [2]. Peri-implantitis is diagnosed when the inflamed mucosa is accompanied with bone loss around the dental implant [3]. If peri-implant mucositis is left untreated, it can result in the progressive destruction of the marginal bone around the dental implant, which in turn leads to peri-implantitis [4,5].
The presence of plaque around dental implants appears to be associated with peri-implant mucositis [6]. Peri-implant lesions are associated with inadequate plaque control at implant sites, whereas peri-implantitis is rare when proper plaque control is ensured [7,8]. In a long-term clinical study, peri-implant lesions were frequently found in patients who did not adhere to supportive therapy, including the removal of bacterial biofilm [6]. Most practitioners agree that the long-term success of implant restorations can be improved by maintaining good oral hygiene and preventing plaque accumulation around the implants [9,10].
Daily plaque control using a manual toothbrush is one effective way to prevent plaque accumulation around teeth [11]. Dental floss and interdental cleansing devices are also recommended for daily plaque control. In some clinical situations, in which an implant-supported prosthesis does not have the proper contour, angulation, or location, more time and effort are required for the daily removal of plaque [12]. Powered toothbrushes may assist in maintaining good oral hygiene, as they provide patients with an easy plaque control technique that does not require substantial training [13].
Powered toothbrushes have advantages compared to other oral hygiene appliances. Sicilia et al. [14] reported that the use of powered toothbrushes, especially those with counter-rotational and oscillating-rotating brushes, can be beneficial in reducing the levels of gingival bleeding or inflammation. Vandekerckhove et al. [13] reported that powered toothbrushes are effective, safe and comfortable for patients who have undergone rehabilitation with implant prostheses. Wolff et al. [15] demonstrated that sonic brushing is an effective means of dental implant maintenance. On the other hand, Swierkot et al. [16] found no significant differences between manual and sonic-powered toothbrushes regarding plaque removal around dental implants. These results were obtained from subjects without periodontal or peri-implant disease. To the best of our knowledge, no studies have evaluated the effectiveness of sonic-powered toothbrushes for plaque removal in subjects with peri-implant mucositis.
The aim of this study was to evaluate the effectiveness of powered toothbrushes, in comparison with manual toothbrushes, for plaque control in patients with peri-implant mucositis.
MATERIALS AND METHODS
Experimental design
This randomized, prospective, controlled, clinical parallel study compared the efficacy of manual toothbrushes (Butler GUM 311, Sunstar, Etoy, Switzerland) and sonic-powered toothbrushes (Sonicare DiamondClean, Philips, Amsterdam, Netherland) for plaque control around dental implants. The sonic-powered toothbrush used in this study has a frequency of up to 31,000 brush strokes per minute and a two-minute timer to ensure the recommended brushing time. The study protocol was approved by the Institutional Review Board (IRB #CMP13003), Seoul National University Dental Hospital, Seoul, Korea. All patients received a detailed description of the proposed study protocol and provided informed written consent to participate in the study. Subjects were recruited from December 2013 to August 2014. The first procedure was carried out in December 2013, and all one-month follow-up visits were completed by October 2014. A block randomization sequence was used to ensure equal distribution of the subjects to the manual toothbrush group and the sonic-powered toothbrush group. The randomization was performed on the day of scaling, using a sealed envelope containing the allocated toothbrush procedure.
The sample size was determined to be 20 subjects per group. Wolff et al. [15] demonstrated that a change of 0.1 (±0.1) in the modified sulcus bleeding index (mSBI) around the implant sites was found between baseline and 24 weeks of follow-up. In our study, a difference of 0.3 in the magnitude of mSBI change after two months was considered to be the threshold of clinical relevance when comparing the use of manual and sonic-powered toothbrushes. A total sample size of 36 subjects (18 per group) was found to achieve 81% power in detecting a difference of 0.3 between the mean mSBI values of the manual toothbrush group and the sonic-powered toothbrush group, with a standard deviation of 0.3. The Mann-Whitney U test was used, and P-values <0.05 were considered to indicate statistical significance. Assuming a drop-out rate of 10%, a total sample size of 40 (20 per group) was required.
Population screening
Patients with bleeding on probing, no residual pocket depth (as shown by a pocket probing depth ≥5 mm), and no radiological peri-implant bone loss were considered eligible for this study. In order to be eligible for enrollment, all the patients had to meet the following inclusion and exclusion criteria.
The inclusion criteria of this study were: 1) the presence of at least one implant restoration, 2) no use of antibiotic medications within the previous three months, 3) the presence of an implant prosthesis that was installed at least three months previously, and 4) no peri-implant bone loss as shown by radiography.
The exclusion criteria of this study were: 1) pregnancy, being less than three months postpartum, bleeding disorders, hemophilia, diabetes, immunodeficiency, epilepsy, rheumatic heart disease, or a joint replacement prosthesis; 2) the use of cyclosporin, dilantin, calcium channel blockers, or the chronic use of non-steroidal anti-inflammatory drugs; 3) the requirement of dental treatment due to dental caries, abscesses, or similar conditions; 4) the presence of an orthodontic appliance; and 5) the presence of a condition that would prevent a patient from actively controlling oral hygiene, such as Parkinson's disease or mental retardation.
Procedures
All subjects were instructed to brush their teeth and implants three times a day for two minutes. Subjects in the manual toothbrush group were instructed to brush their teeth and implants using the Bass technique [17], and subjects in the sonic-powered toothbrush group were told to follow the manufacturer's instructions.
Clinical baseline measurements were taken at the screening appointment, along with a standard periapical radiograph in order to exclude peri-implantitis. The data included the modified plaque index (mPI), mSBI [18], and clinical photographs (buccal and lingual views). Clinical measurements were taken by blind and calibrated investigators. Scaling was performed to minimize the effect of natural teeth adjacent to the implant at the first visit. The data were uploaded to a database in which patient privacy was protected according to current regulations. Clinical parameters were recorded at baseline as well as at one-month and two-month follow-up visits.
Patients were requested to complete a questionnaire that assessed oral hygiene habits and patient compliance. The duration and frequency of tooth brushing were recorded by the subjects for compliance assessment.
Statistical analysis
After a brief training, two examiners (JWL, JEL) performed repeated measurements of the mPI and mSBI using clinical photographs one week apart. The intra-examiner reproducibility and inter-examiner reliability of the measurements of the mPI and mSBI were assessed using the intraclass correlation coefficient and Kappa statistics [19,20].
The Student's t-test (for continuous measures) or the Mann-Whitney U test (for categorical measures) was used to evaluate whether any statistically significant differences were present between the two groups at each time point, and the Wilcoxon signed-rank test was used to evaluate whether statistically significant changes occurred from baseline within each group. P-values <0.05 were considered statistically significant. Correlations between the age of subjects and the change of the mPI and mSBI were determined with the Spearman's correlation test. All statistical analyses were performed using IBM SPSS Statistics version 21.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Subject data
The initial study population consisted of 41 volunteers who were recruited from the patients of Seoul National University Dental Hospital. One subject withdrew consent to participate in the study, resulting in a total of 40 participants who participated in the study (Table 1). The subjects of the manual toothbrush group ranged in age from 39 to 75 years (mean±standard deviation [SD]=54.5±10.6 years) and included 11 men and nine women. The subjects of the powered toothbrush group ranged in age from 27 to 75 years (mean±SD=54.6±11.7 years) and included 12 men and eight women. A total of 33 implants were present in the manual toothbrush group, and 30 implants were present in the powered toothbrush group. The time of implant restoration ranged from 2.7 to 9.0 years (mean±SD=5.6±2.8 years) in the manual toothbrush group and from 3.2 to 8.1 years (mean±SD=4.8±2.9 years) in the powered toothbrush group. The time of implant placement ranged from 3.0 to 9.6 years (mean±SD=6.4±3.1 years) in the manual toothbrush group and from 3.6 to 8.7 years (mean±SD=6.2±2.5 years) in the powered toothbrush group.
Subject oral hygiene habits and compliance
The data collected from the questionnaire relating to oral hygiene habits and compliance are shown in Table 2. The daily frequency of brushing in the manual toothbrush group was significantly higher than in the powered toothbrush group, whereas the duration of brushing in the manual toothbrush group was significantly shorter than in the powered toothbrush group at one and two months of follow-up. The frequency of use of an interdental brush and dental floss in the manual toothbrush group was comparable to that found in the powered toothbrush group. At one month and two months of follow-up, larger differences were found between the two groups. The percentage of patient compliance was significantly different between the two groups at one month of follow-up, but not at two months.
Intraexaminer and interexaminer reliability
The intraexaminer evaluation yielded high reproducibility, with intraclass correlation coefficients for JWL and JEL of 0.941 and 0.912, respectively. The interexaminer evaluation likewise yielded high reliability, with a kappa value for JWL and JEL of 0.91.
Clinical parameters at the implant sites
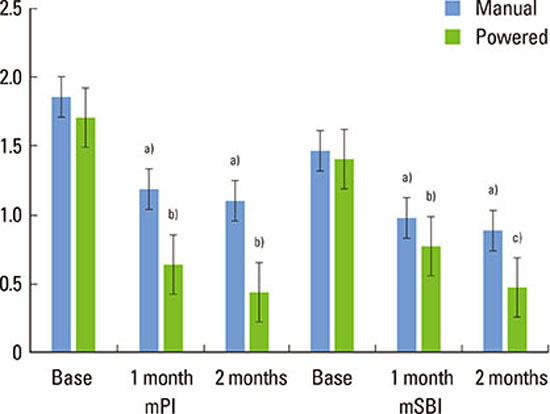
The mPI and mSBI scores were observed in the manual and powered toothbrush groups at baseline and at one and two months of follow-up. In the manual toothbrush group, the mean±SD mPI scores at the baseline, one month, and two months were 1.85±0.62, 1.18±0.98, and 1.09±0.95, respectively. In the powered toothbrush group, the corresponding mPI values were 1.70±0.65, 0.63±0.72, and 0.43±0.68, respectively. A significant difference in the mPI values of the manual and powered toothbrush groups was found at two months of follow-up.
An overall pattern in which mPI and mSBI values decreased post-baseline was observed in both groups (Table 3). In both groups, statistically significant reductions of mPI and mSBI values were found at one month and two months of follow-up compared to the baseline values. Moreover, in the powered toothbrush group, a statistically significant reduction in the mSBI was found between one and two months of follow-up (Fig. 1). The overall reductions were not significantly different between the two groups, except the mPI reduction between baseline and two months of follow-up (Table 3). The Spearman coefficients between age and the change of mPI and mSBI (from baseline to two months of follow-up) were -0.209 (P-value=0.244) and -0.102 (P-value=0.508) in the manual toothbrush group and -0.044 (P-value=0.818) and -0.034 (P-value=0.860) in the powered toothbrush group, respectively.
DISCUSSION
The results from the present study have demonstrated that the use of both manual and powered toothbrushes led to significant reductions in mPI and mSBI scores. However, no significant differences were found between the two groups for any post-baseline metric except mPI at two months of follow up. This finding could be due to a therapeutic effect and a genetic effect. Professional scaling was performed at the first visit to minimize plaque that had accumulated around the natural teeth and the dental implant, because the presence of bacterial plaque could have affected the clinical parameters evaluated in this study. Oral hygiene education was also performed at the first visit, because the subjects had not undergone recent oral hygiene education at the same time point before the study. Professional scaling and oral hygiene education could conceal the differences between manual and powered toothbrushes in a relatively short-term study, in which the therapeutic effect could be substantial [14,21]. Unlike short-term studies, long-term studies have reported significant differences in gingival bleeding depending on the use of manual or powered toothbrushes [21,22]. Therefore, if we had investigated the subjects in a long-term study, it is probable that differences in the mPI or mSBI values would have been observed. Another factor leading to these results is the possible effect individual genetic factors on host immunity [23,24]. Depending on individual genetic factors, the inflammatory response of soft tissue to bacterial plaque could be different. Therefore, genetic factors could affect the variation of parameters such as mSBI between the two groups. A larger sample size would probably be necessary to rule out such differences.
Various types of powered toothbrush motion exist, including side to side, counter-oscillation, rotation oscillation, circular, sonic, and ionic. The powered toothbrush provided to the subjects in this study was a sonic toothbrush that uses high-velocity lateral vibrations. In their review study, Yaacob et al. [25] reported that sonic toothbrushes reduced plaque and gingivitis more than manual toothbrushes. In another review study, sonic toothbrushes were found to be inferior to rotation/oscillation-powered toothbrushes for removing plaque, especially from tooth surfaces that are difficult to clean, such as the lingual and proximal surfaces [26]. Based on previous studies and the present study, we can conclude that sonic-powered toothbrushes have a positive effect on plaque control, even if it has not been shown that they are superior to other types of powered toothbrushes.
Biofilm overgrowth in the peri-implant pocket contributes to the increase of inflammatory mediators, such as matrix metalloproteinases and interleukins. Assessing changes of both clinical and biological parameters over time would enable a more thorough evaluation of the effectiveness of manual and powered toothbrushes in peri-implant mucositis patients. In particular, cytokine levels should be evaluated in future studies, in addition to mPI and mSBI values.
Powered toothbrushes can be especially useful for geriatric patients with impaired manual skills. Verma and Bhat [27] compared the efficacy of manual and powered toothbrushes in patients aged 68-85 years. They reported that powered toothbrushes were more effective than manual toothbrushes in removing plaque and controlling gingivitis. However, in the present study, the age of the patient was not found to contribute significantly to the change of mPI or mSBI from baseline to two months of follow-up. Both the manual and powered toothbrush groups contained only three elderly subjects (with an age > 65 years). More elderly subjects should be recruited in future studies in order to identify the relationship between age and the change of mPI and mSBI values in response to treatment.




 XML Download
XML Download