

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recent technological advances have led to the ongoing development of novel approaches to the treatment of peri-implantitis [1]. Peri-implantitis is an inflammatory process affecting the tissue around an osseointegrated implant, resulting in the loss of supporting bone due to specific anaerobic bacteria [2]. Microbiological findings in failing implants suggest that bacteria implicated as pathogens in periodontitis may play a role in the development of peri-implantitis. Staphylococcus spp., Capnocytophaga, spirochetes, Gram-negative anaerobic rods, Fusobacterium species, Porphyromonas gingivalis, Prevotella intermedia, and Aggregatibacter actinomycetemcomitans have been cultivated from failing implants in greater proportions than would normally be expected [3,4,5,6,7,8,9].
Various methods have been advocated for the treatment of peri-implantitis. Therapies that have been proposed include flap surgery, debridement of the implant surface, chemical conditioning of the implant surface, bone regenerative procedures, and topical or systemic antibiotic and/or antimicrobial therapy [10]. Lang et al. [11] proposed cumulative interceptive supportive therapy for peri-implantitis treatment, and attached great importance to the mechanical cleaning of the implant surface. However, implant surface alterations have been found occur during mechanical cleaning, involving techniques such as the use of an ultrasonic scaler, stainless steel curettes, titanium curettes and an air polishing abrasive system [12]. Implant surface alterations of this type involve the transfer of foreign ions into the oxide titanium layer and lead to reduced biocompatibility. Several studies have established the bactericidal effects of high-energy lasers on contaminated implant surfaces [13,14]. After irradiation with certain lasers, however, titanium surface alterations have been observed on treated titanium surfaces [15,16,17,18].
Due to the increasing need for the safe and effective treatment of peri-implantitis, more attention has been focused on non-invasive photodynamic therapy (PDT) in the treatment of peri-implantitis [1]. Even though the original technique was first applied to the treatment of cancer, during the last decade, an increasing number of studies have evaluated the application of PDT in periodontics. Studies have found that periodontal pathogens may be effectively eliminated using PDT, which combines the application of a nontoxic chemical agent (the photosensitizer) with low-level light energy. PDT has been considered a promising novel therapeutic approach for the elimination of pathogenic bacteria in periodontal and peri-implant diseases. PDT essentially involves three nontoxic components: harmless visible light, a nontoxic photosensitizer, and oxygen. It is based on the theory that the photosensitizer adheres to the target cells and can be excited by light of a suitable wavelength. Following the activation of light at a certain wavelength, singlet oxygen and other very reactive agents are produced, and these products are mortally toxic to certain cells and bacteria.
Laser light has been found to be very effective in cleaning various surfaces in vitro, as described by several authors. Haas et al. [19] assessed the efficacy of PDT in killing bacteria associated with peri-implantitis, such as A. actinomycetemcomitans, P. gingivalis, and P. intermedia, which were adhered to titanium plates with different surface characteristics (a machined surface, a titanium plasma-flame-sprayed surface, a sand-blasted surface, and a hydroxyapatite surface). None of the smears acquired from the plates subjected to PDT expressed bacterial growth of any of the microorganisms. Scanning electron microscopy (SEM) images showed that antimicrobial PDT induced bacterial cell destruction without damaging the titanium surface.
Several implant surface treatment techniques have recently been developed with the goal of improving the outcomes of dental implantation. Among these methods, sand-blasted, large-grit, acid-etched (SLA) and resorbable blasted media (RBM) surfaces have been used widely and have shown successful long-term results. However, increased surface roughness after the SLA and RBM treatments can lead to greater bacterial adhesion. It has been established that bacterial adhesion on implants influences peri-implant inflammation. However, the effect of PDT on bacteria associated with peri-implantitis that have been adhered to RBM and SLA surfaces of dental implants has not yet been examined. Therefore, this study aimed to assess the efficacy of PDT using erythrosine and a green light emitting diode (LED) light source on biofilms of A. actinomycetemcomitans attached to RBM and SLA titanium surfaces in vitro.
MATERIALS AND METHODS
Preparation of the titanium disks
Titanium disks were manufactured with a diameter of 8 mm and a thickness of 1 mm, and underwent either RBM or SLA surface treatment. One side of each disk was covered with regular hydrophilic vinyl polysiloxane impression material (GC Corporation, Tokyo, Japan) and baseplate wax (Kim's International Inc., Seoul, Korea) before bacterial inoculation. The disks were sterilized by being dipped in 70% ethanol and were dried before the experiment.
Bacterial strains and culture conditions
5 ATCC 33384, obtained from a Korean collection of specimens relevant to oral microbiology (Chosun University, Gwangju, Korea) were used. A. actinomycetemcomitans was cultivated for one day in trypticase soy broth (Becton, Dickinson and Company, Sparks, MD, USA), yeast extract, 5 mg/mL of hemin (Sigma Chemical Co., St. Louis, MO, USA) and 1 mg/mL of menadione (Sigma Chemical Co., St. Louis, MO, USA) under anaerobic conditions (Bactron Anaerobic Chamber, Sheldon Manufacturing Inc., Cornelius, OR, USA) with an atmosphere of 90% N2, 5% CO2, and 5% H2.
The next day, 2 mL of culture medium and 50 µL of bacterial culture medium were inoculated in 24-well culture plates (Corning Inc., NY, USA) for 72 hours in anaerobic conditions together with the titanium disks.
Scanning electron microscope
After incubating disks at 37℃ in bacterial culture medium inoculated with A. actinomycetemcomitans for 72 hours under anaerobic conditions, the disks were washed twice with phosphate-buffered saline (PBS). The experiments were performed in 24-well culture plates.
Disks with attached bacteria were fixed in 2.5% glutaraldehyde in PBS (pH 7.4) for one hour at room temperature. The fixed samples were then washed three times with PBS for 10 minutes and dehydrated for 30 minutes in a graded series of ethanol. After critical point drying, the samples were mounted on stubs, coated with gold, and observed with SEM.
The RBM and SLA surfaces of the disks were examined by SEM (10,000× and 30,000×). Variable-pressure field emission SEM (SUPRA55VP, Carl Zeiss, Oberkochen, Germany) was used to examine the bacteria attached to the titanium disks.
In order to confirm bacterial detachment from the titanium surfaces, the surfaces of the titanium disks were examined with SEM after agitating the disks with attached bacteria in a glass tube with PBS and sterile glass beads (Ø 0.15 mm, Daihan Scientific, Wonju, Korea) by vortexing for 60 seconds with a vortex mixer (N-BIOTEK, Bucheon, Korea).
Photodynamic therapy
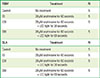
After incubating for 72 hours, all disks were then rinsed twice with PBS. The RBM and SLA disks were subdivided into four groups, including one control group and three test groups, reflecting three different PDT protocols for each surface (Table 1). A total of eight groups were used in this study. Each group consisted of five disks.
The disks belonging to the control group, in which no treatment was applied, were put into a test tube and agitated with 500 µL of PBS and small glass beads for 60 seconds. The disks in the E0 group were put into 500 µL of 20 µM erythrosine for 60 seconds, after which each disk was put into a test tube and agitated with PBS and glass beads for 60 seconds. The disks in the E30 group were put into erythrosine for 60 seconds, and then irradiated with an LED (Photron Co. Ltd., Seoul, Korea) with a spectrum of emission ranging from 520 to 530 nm for 30 seconds (150 mW/cm2, 4.5 J/cm2). The light beam irradiation diameter was 6 mm, and the distance between the light source and the exposed disk surface was 10 mm.
After irradiation, each disk was put into a test tube and agitated with PBS and glass beads for 60 seconds to detach the bacteria from the titanium disk. The disks in the E60 group were put into erythrosine for 60 seconds, and then irradiated with an LED for 60 seconds (150 mW/cm2, 9 J/cm2); after irradiation, each disk was put into a test tube and agitated with PBS and glass beads for 60 seconds.
In order to characterize changes in the appearance of bacteria on the disk surfaces after PDT, the disks in the E60 group were examined by SEM (10,000× and 30,000×).
After agitation, 200 µL of solution containing detached bacteria was spread directly on brucella blood agar plates (10.0 g/L of enzymatic digest of casein, 10.0 g/L of enzymatic digest of animal tissue, 2.0 g/L of yeast extract, 1.0 g/L of dextrose, 5.0 g/L of sodium chloride, 0.1 g/L of sodium bisulfide, 5 mg/L of hemin, 0.01 g/L of vitamin K1, 15.0 g/L of agar, 50 mL/L of sheep blood) (Hanil-KOMED, Seongnam, Korea) by using a spiral plate system (IUL, Barcelona, Spain).
The plates were incubated in anaerobic conditions (90% N2, 5% H2, 5% CO2) for 72 hours at 37℃. The number of colony-forming units (CFUs) was determined by an automatic colony counter (IUL, Barcelona, Spain). The survival rate of the bacteria was determined by counting the CFUs after incubation. The data were expressed as the percent survival of bacteria after PDT. The percent survival of bacteria was calculated by dividing the CFUs on the test group disks by the CFUs on the non-treated controls.
Confocal laser scanning microscopy
A time-resolved fluorescence confocal microscope (MicroTime-200, Picoquant, Berlin, Germany) was used to observe the distribution of live and dead microorganisms on the disk surfaces. Additional disks from each group, including the control group, were prepared in order to produce specimens. The disks were attached to a glass slide and then stained with SYTO 9 and propidium iodide, using the LIVE/DEAD BacLight Bacterial Viability Kit (Molecular Probes, Inc., Eugene, OR, USA) in the dark at room temperature for 15 minutes. Then, the reagent was removed, and the glass slips were cautiously washed with distilled water and examined at a magnification of 400× through a CLSM [20].
Excitation was performed at a wavelength of 485±14 nm. Emitted fluorescent light was collected by two separate emission filters at 500 nm (SYTO 9) and 635 nm (propidium iodide). Image-processing techniques were used to assess the distribution of live and dead microorganisms.
Data analysis
All analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). The Kruskal-Wallis test was used to determine whether a statistically significant difference was present based on the LED exposure time and application of erythrosine, and the Mann-Whitney U-test using Bonferroni correction was then employed to adjust the P-value. Thus, the threshold for statistical significance was set at P<0.0083.
RESULTS
Scanning electron microscope
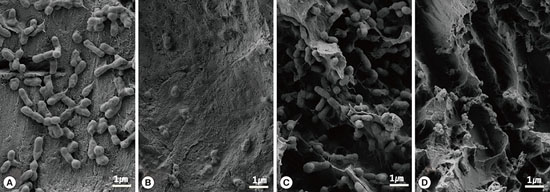
Fig. 1A and 1C show SEM images of surface-modified titanium covered by A. actinomycetemcomitans. Most of the RBM and SLA titanium surfaces were covered with one or two layers of microbes. After agitation, a titanium surface image was obtained by SEM to identify bacterial detachment. Compared to the image before agitation, a significant amount of bacteria was detached from the titanium surface (Fig. 1B and D).
On the SEM images, the SLA surfaces were found to be rougher than the RBM surfaces and more bacteria were attached in the deep valley areas of the titanium surfaces.
Fig. 2A to 2D show SEM images illustrating changes in the appearance of A. actinomycetemcomitans before and after PDT, demonstrating that the outer walls of the bacteria were damaged without alterations to the titanium surface.
Determination of bacterial survival
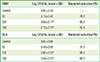
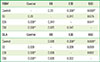
Tables 2 and 3 show the mean log CFU/mL of bacteria and the percentage of bacterial reduction in the RBM and SLA disks, depending on the treatment group. The mean log CFU/mL values of the E30 and E60 groups were lower than the control group. In the RBM group, 92.4% of bacteria were removed in the E60 treatment group. The E60 treatment group of the SLA disks showed an 88.9% reduction.
Statistical significance was found among the treatment groups (P<0.05), indicating the presence of significant differences among the control, E0, E30, and E60 groups in both the RBM and SLA disks. A significant reduction was found in the log CFU/mL value of the RBM and SLA surface groups (Tables 2 and 3).
In both surface groups, significant differences were found between the control group and the E30 and E60 groups (P=0.008). The E30 and E60 groups showed lower log CFU/mL values, and the E60 group showed the greatest magnitude of bacterial reduction.
Confocal laser scanning microscope
Confocal scanning laser microscopy images obtained from the titanium surfaces showed a mixture of live and dead microbes (Fig. 3). The control and E0 groups in both the RBM and SLA groups showed a high proportion of live bacteria, which had a green color, however, in the images of the E30 and E60 group, a qualitatively tendency for more dead bacteria, which had red color, to be present was noted.
DISCUSSION
This study was designed to observe the effect of PDT using green light LED and erythrosine on biofilms of A. actinomycetemcomitans on surface-modified titanium in vitro.
Peri-implantitis is an inflammatory process affecting the tissues around an osseointegrated implant, resulting in the loss of supporting bone due to various anaerobic bacteria. Mobelli et al. [21] determined that the bacteria associated with peri-implantitis are anaerobic bacteria such as P. gingivalis, A. actinomycetemcomitans, P. intermedia, and spirochetes.
Dörtbudak et al. [22] described PDT using toluidine blue O (TBO) and diode soft lasers (690 nm) on implant surfaces (plasma-sprayed coated IMZ®, Friedrichsfeld AG, Mannheim, Germany). The results of this in vivo study found that PDT on implant surfaces involved in peri-implantitis is valuable in reducing P. gingivalis, A. actinomycetemcomitans, and P. intermedia, although complete elimination of the bacteria was not achieved. Bürgers et al. [23] studied biofilm formation on two different titanium implant surfaces, including pure machined and SLA titanium specimens. The in vitro and in vivo tests showed that the SLA surface had a significantly higher surface roughness and a higher level of bacterial adhesion than the machined surface. They concluded that the initial bacterial adhesion to different titanium surfaces is influenced by surface roughness. Song et al. [24] found SLA titanium surfaces to have higher levels of surface roughness than RBM surfaces. In the present study, SEM images of bacterial adhesion to the disk surfaces showed that A. actinomycetemcomitans attached well to rough surfaces, such as those created by SLA and RBM treatment. In the SEM images, more surface valleys were found on the SLA surfaces than on the RBM surfaces. Marotti et al. [25] used a low-level GaAlAs diode laser and a methylene blue photosensitizer in PDT on anodized implant surfaces in vitro. The results of their study suggested that PDT on contaminated implant disks was efficient, whereas laser irradiation without a photosensitizer was less efficient than PDT.
In this study, we studied A. actinomycetemcomitans, which is a species of anaerobic bacteria associated with peri-implantitis, and evaluated the effect of PDT in which a green light LED and erythrosine were used. The data from our study indicate that PDT with erythrosine and a green LED light source (520 nm) administered for 30 and 60 seconds resulted in significant bacterial reduction. On the RBM surfaces, the initial bacterial CFU/mL value was reduced by 76.5% in the E0 group, 85.6% in the E30 group, and 92.4% in the E60 group. On the SLA surfaces, the initial bacteria CFU/mL value was reduced by 31.2% in the E0 group, 88.6% in the E30 group, and 88.9% in the E60 group. The results from the RBM and the SLA surface groups demonstrated that exposure to the dye with or without LED irradiation was effective in reducing the viable bacterial number of A. actinomycetemcomitans. However, subsequent irradiation with LED light was more effective in reducing the viable bacterial number of A. actinomycetemcomitans. After PDT, the outer walls of bacteria were damaged, as observed by SEM. Thus, using a photosensitizer with a light source is more effective than using a photosensitizer alone. However, complete bacterial elimination was not found in any group.
No significant difference was found between the groups that underwent 30 and 60 seconds of irradiation. This result implies that irradiation with a LED for more than 30 seconds does not lead to more effective bacterial reduction on SLA titanium surfaces.
In most studies, PDT on the implant surface has been performed with laser irradiation and TBO [19,22,26,27,28,29]. These studies have shown that PDT with diode laser irradiation and TBO is effective in reducing the bacterial count. Low levels of diode laser irradiation did have an adverse effect on the titanium surfaces. Moreover, the application of diode lasers in clinical settings requires expensive equipment to treat peri-implantitis with PDT. LED devices, however, are more compact, inexpensive, and portable than lasers.
In the present study, erythrosine was used as a photosensitizer for PDT. Erythrosine is currently used to stain and visualize dental plaque. It has been reported to have antimicrobial activity against Gram-positive and Gram-negative oral bacteria [30,31,32]. Erythrosine absorbs light in the visible range, and has the ability to initiate photochemical reactions. Wood et al. [33] and Metcalf et al. [34] have demonstrated that erythrosine is an effective photosensitizer for killing the cariogenic bacterium Streptococcus mutans in erythrosine-mediated PDT. Lee et al. [35] demonstrated that PDT with 3 W LED irradiation using erythrosine had a suppressive effect on Streptococcus sobrinus, particularly in green light (520-530 nm). The maximum absorption wavelength for erythrosine is 500-550 nm, and in this study, a green LED light (520-530 nm) was used to ensure optimal absorption. High-energy laser irradiation was not used to activate the photoactive dye because relatively low-level exposure produces a high bactericidal effect [1]. Qin et al. [36] carried out PDT using TBO and 635-nm laser light on periodontal pathogens. The results of their study showed that the maximal bactericidal effect was detected when light intensity was increased to 159 mW/cm2, which led to as effective a bactericidal effect as that observed at 212 mW/cm2. However, they noted that the most significant determinant of the bactericidal effect was the total light dose received by the bacteria treated with TBO. When the light dose increased from 0 to 12 J/cm2, the bacterial survival rate decreased markedly. This may be because the number of photons absorbed by the photosensitizer increased with the increase in light dose. The LED light intensity used in our study was 150 mW/cm2, which is a low level of energy, and the light dose was 0, 4.5, and 9 J/cm2 in the various groups. The survival rate of the bacteria decreased markedly when the light dose increased from 0 to 4.5 J/cm2. However, at more than 4.5 J/cm2, PDT did not show an increasing bactericidal effect. This may be explained by the fact that enough photons were supplied to the molecules contained in the 500 µL solution of 20 µM erythrosine to ensure complete activation. As a result, no significant difference was observed between the E30 and E60 groups.
Geminiani et al. [37] found that 810-nm diode laser irradiation applied for 14 seconds to implant surfaces increased the surface temperature by 10℃. Heat production that causes the temperature to rise above 47℃ for 60 seconds negatively affects living bone and compromises its regeneration [38]. Since the LED light used in this study utilizes low levels of energy, there is no danger of adverse effects to the titanium surface.
The results of this study show that LED green light with erythrosine is an effective combination for PDT performed to eliminate A. actinomycetemcomitans attached to titanium surfaces. However, this study has some limitations. First, the complete elimination of the bacteria was not achieved under the in vitro conditions of this study. Therefore, further research is needed to determine the optimal combination of the photosensitizer (agent concentration and agent exposure time) and light source (laser power energy, irradiation time) for PDT performed to eliminate A. actinomycetemcomitans biofilms on titanium surfaces. Second, this study is an in vitro experiment, testing conditions that are very different from those found in vivo. Biofilms in the oral cavity have a complex composition, consisting of multiple species of bacteria and their byproducts. Therefore, findings regarding the removal of A. actinomycetemcomitans by PDT cannot be directly applied to in vivo situations. Additional in vivo research is needed to apply this technology clinically.
Within the limits of this study, PDT using erythrosine and a green LED with a wavelength of 520-530 nm, a light intensity of 150 mW/cm2, and a light dose of 4.5 J/cm2 was effective in reducing the viability of A. actinomycetemcomitans attached to surface-modified titanium in vitro.



 XML Download
XML Download