

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary implant stability is typically defined as the stability of an implant immediately after its placement. Primary implant stability is a prerequisite for obtaining adequate osseointegration of dental implants and is considered an important predictor for successful osseointegration [1]. Without primary stability, the implant can become surrounded by fibrous encapsulation [2]. A lack of primary stability seems to be one of the leading causes of early implant failure.
The degree of primary stability achieved is influenced by numerous factors, including the bone quality and quantity, implant geometry, implant surface characteristics, surgical technique, and operator skills [3,4,5,6,7,8,9]. Cortical bone is the main structure that provides implant stability during surgery and resists the axial loading of an osseointegrated implant [10]. One study reported the use of dental implant bone cement to provide early implant stability in a loosely prepared bony socket. The mechanical properties and secondary stability of the bone-cement-implant interfaces of implants were found to be superior to those of the self-threaded implants throughout one to 12 weeks of healing. Roze et al. [7] showed a significant correlation between implant stability quotient (ISQ) values and the cortical bone thickness measured with a computed tomography scan. Moreover, our previous study showed that thin cortical bone thickness was associated with a low ISQ value [11]. The ISQ measuring direction also influenced the ISQ values.
Bone cement is composed of 100% pure synthetic β-tricalcium phosphate (β-TCP) bone filler or bone substitute that contains a polyphosphate, which is an osteogenesis stimulating factor. It has a macroporous structure that enables blood vessels and/or bones to grow inside it. After approximately seven weeks, the commencement of absorption can be identified. Bone cement is commonly employed in orthopedic surgery and neurosurgery [12,13,14]. The ideal hardening time of bone cement is less than 5 minutes, and this reaction is not an exothermic reaction. Furthermore, multilayer augmentation is possible in most cases.
For dental implants, the initial stability of the implant is dependent on the presence of a sufficient amount of cortical bone in the implant bed. Therefore, to improve the initial stability of implant, especially in patients with insufficient cortical bone, bone cement can be used as the bone graft material. The objective of the present study was to evaluate the effect of bone cement grafting on the initial stability of a bone implant in an area with insufficient cortical bone.
MATERIALS AND METHODS
Drilling procedure and defect preparation
The defect was prepared following our previously described procedure [11]. Six frozen bovine rib bones from a Korean bull or cow were used in this study. For thawing, the frozen bovine rib bones were left at room temperature for 3 hours before performing the experiment. To allow for the creation of an 8-mm diameter defect, bovine rib bones with minimum width of 8 mm were used. Seven implant beds were prepared in each rib bone, and the centers of the implant beds were 15 mm apart. The drilling sequence recommended according to the manufacturer's protocol (Shinhung Co., Seoul, Korea) was modified to accommodate the thick cortical bone in bovine rib bones; our drilling sequence was a 2.0-mm drill, 2.4-/2.8-mm drill, 3.2-/3.6-mm twist drill, and 4.0-mm tap drill.
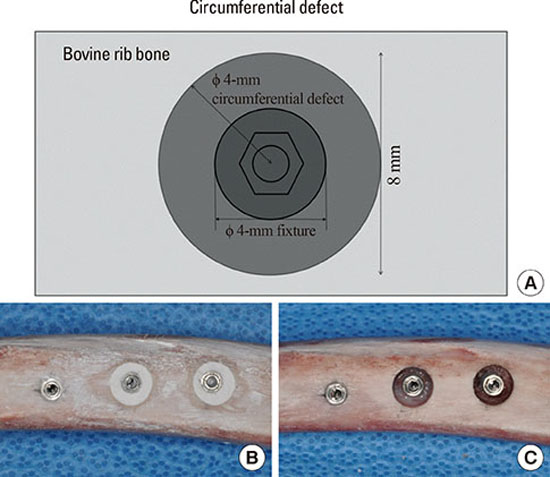
Two kinds of circumferential defects were made: the first was 8 mm in diameter and had a depth of 2.5 mm, and the second was 8 mm diameter and had a depth of 5.0 mm. The control area had no defect (Fig. 1A and B). For each of the two defect groups and the control group, 14 samples were prepared for each group. The circumferential defect was made around the prepared drilling hole using a trephine bur 8 mm in diameter. After drilling with the trephine bur, bone was removed using a #770 bur to create the 2.5-mm or 5-mm depth in the circumferential defect (Fig. 1B). After preparation of the bone defects, the cortical bone thickness was measured using a UNC-15 probe. In this bovine bone model, we considered the area outside of the rib arch as the buccal side and the area inside of the rib arch as the lingual side. In addition, the left side was considered the mesial side, and the right side was considered the distal side.
Implant placement and ISQ measurement
In the six bovine rib bones used in our study, seven implants were placed in each bone. These implants were external connection-type implants (φ 4 mm×10 mm) (Sola, Shinhung Co.) and were placed in each prepared hole. Each implant fixture had a platform diameter of 4.1 mm, with a height of 0.7 mm (the hexagonal connection), a pitch length of 6 mm, and a self-tapping fixture design. ISQ values were measured three times from the four directions (mesial, distal, buccal, and lingual sides) with an Osstell instrument (Integration Diagnostics AB, Göteborg, Sweden). After measuring the ISQ values, the bone cement (Polybone, Hanmi Medicare Inc., Seoul, Korea) was mixed for 30 seconds, allowed to react for 10-30 seconds, and then grafted into each prepared circumferential bone defect (Fig. 1C), which took approximately 4 minutes. After grafting, the cement was allowed to harden for 3 minutes. Last, the ISQ values were measured again.
Statistical analysis
Differences in the thickness of the cortical bone and the ISQ values between all three groups were analyzed using one-way analysis of variance with the Tukey test. The differences in the ISQ values before and after bone cement placement were analyzed using paired t-tests. The significance level of these tests was determined at P<0.05. All statistical calculations were performed using PASW Statistics ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
The thickness of the cortical bone before drilling in the control, circumferential 2.5-mm defect, and circumferential 5-mm defect groups were 2.75 mm, 2.68 mm, and 2.86 mm, respectively (P>0.05) (Table 1). After preparation of the bone defect, no cortical bone remained in the 5-mm defect group, and only a thin layer of cortical bone remained in the 2.5-mm depth group. The ISQ values before and after bone cement grafting are shown in Table 1. Before bone cement grafting, the ISQ values varied largely across the defect depth groups. As the defect depth increased, the ISQ value decreased. In the controls, the ISQ value was 85.45±3.36 (mean±standard deviation). In the 2.5-mm and 5-mm defect groups, the ISQ values were 69.42±7.06 and 57.43±6.87, respectively, before bone cement grafting. These three values were significantly different from one another (P<0.001). After bone cement grafting, the ISQ values increased to 73.72±8.00 and 67.88±10.09 in the 2.5-mm (P<0.05) and 5-mm defect groups (P<0.001), respectively. Although the ISQ value in the 5-mm defect group was lower than that in 2.5-mm defect group, the difference between the ISQ values before and after grafting were greater in 5-mm defect group than that in the 2.5-mm defect group was.
The ISQ values were measured from four directions to evaluate whether these values differed depending upon the measuring direction. For all measuring directions, the ISQ values decreased as the defect depth increased (Table 2). After grafting the bone cement in the 5-mm defect group, the ISQ value in buccal direction was the highest, and then decreased in the order of the distal, lingual, and mesial direction (P<0.05). Moreover, all of the ISQ values before and after grafting were statistically significant except for those in the lingual direction. After grafting, none of the ISQ values in the 2.5-mm and 5-mm defect groups was statistically significant except for those in the mesial direction.
The ISQ values were then categorized as being measured perpendicular to the rib bone or parallel to the rib bone (Table 3). The buccal and lingual directions were considered as perpendicular to the rib bone axis, and the mesial and distal directions were considered as parallel to the rib bone axis. The ISQ values did not significantly differ between these two different directions. When the ISQ values were compared before and after grafting, they were found to be significantly greater after bone cement grafting. In the 2.5-mm defect group, the ISQ values measured in the parallel and perpendicular directions increased from 68.88 and 69.95 before grafting to 73.30 and 74.14 after grafting, respectively. Likewise, in the 5.0-mm defect group, the ISO values measured in perpendicular and parallel directions increased from 56.55 mm and 58.32 mm before grafting to 68.77 mm and 66.98 mm after grafting, respectively.
DISCUSSION
β-TCP has been a used widely graft material in dental, cranial, and spinal surgery [15,16,17,18,19,20]. In addition, cement type bone graft material, which is composed of β-TCP and polyphosphate, has been used to induce bone regeneration after cranial or spinal surgery [12,13,14]. It has also been used as a scaffold because of its high porosity that provides sufficient spaces for newly formed bone to grow after spinal surgery. Moreover, it has been used as a grafting material to fill defects or sinuses in cranial surgery.
The main determinants of implant stability are the mechanical properties of the bone tissue at the implant site and the ability to obtain firm implant engagement with the bone tissue [1,21]. In a previous study that tested the use three different kinds of defects [11], the ISQ value decreased as the amount of cortical bone around the implant decreased. Moreover, a loss of cortical bone reduced the stability of these implants and the ISQ values. The ISQ values of the three-wall defect group (81.74±3.32) did not significantly differ from the no defect (control) group (84.70±5.52). However, the ISQ values for the circumferential and one-wall defect groups were significantly lower than that of the other groups [11]. Another study found the initial implant mobility within the cortical layer to result in a significantly less amount of bone around the implants than that around the stable controls was [22].
Risk factors for the unstable placement of implants include poor bone quality, maxillary posterior jaw locations, and short implants. Implant diameter is not related to primary stability [23]. Herr [24] summarized several methods that increase implant success when the initial stability at the implant placement site is insufficient. First, if the alveolar ridge width and height are sufficient, a longer or wider implant fixture placement should be considered. Second, if the alveolar ridge width and height are insufficient and it is not possible to install a longer and wider implant, extending the time between the first and second surgery or delaying the prosthodontic treatment should be considered to provide more time for osseointegration. Third, the use of a self-tapping implant was recommended to overcome any insufficient initial stability. Fourth, inserting a grafting bone substitute into the preparation hole before implant placement was suggested to improve the primary stability of the implant. Last, the use of a bone cement graft around the prepared implant beds was also recommended as a method to overcome any insufficient initial stability of the dental implant.
In 2011, Seong et al. [10] tested the experimental placement of dental implants with a smaller diameter than the drill used for the preparation of the bone in rabbit tibia. Thereafter, bone cement was grafted into the space between the prepared bone and the placed implants. The bone cement used around the initially unstable dental implants in the rabbit model was found to result in early implant stability and improved mechanical properties of the implant.
In the present study, the ISQ values increased four to 10 points more after bone cement application, which served to increase the initial stability. The ISQ value increased the most in the 5-mm depth defect group. Although the ISQ values after grafting were not as high as that of the control group, a significant increase in the ISQ values of the defect groups was observed. After bone cement grafting, the manipulation of the implant by inserting a cover screw and/or healing abutment connection might be easier than that before grafting is. In addition, measurement of the ISQ level has been found to be influenced by the measurement orientation along the axis of the alveolar ridge [25,26,27]. In a hard jawbone model, the initial measurement of the ISQ values recorded in the parallel orientation was greater than that in the perpendicular orientation. However, these two values did not show any significant difference in the present study; a slight difference was found between the perpendicular ISQ values and that of the parallel ISQ values, but it was not significant.
According to a study by Morris et al. [23], initial implant mobility (the mobility observed at implant placement) was observed in 2.8% of 1,554 placed implants. Implant mobility was the mostly found in the maxillary posterior area that has poor bone density (6.3%). Of the implants placed in D4 bone, 12.2% were found to be mobile at placement, which was higher than the percentage of implants placed in denser bone. Moreover, 97.7% of these mobile implants were stabilized by stage II, the uncovering, was carried out. This promising finding might result from the sufficient healing period. Before abutment connection, implants were allowed to heal for 4-6 months in the mandible and 6.5-8 months in the maxilla. In this study, the direction that the measurement was made did not result in different findings. In our previous study, the direction of the measurement was significantly different in the one- and three-wall defect groups, but did not significantly differ in circumferential defect group.
This study showed that the use of bone cement remarkably increased the stability of implants that otherwise had insufficient stabilities at placement, which was caused by an insufficient volume of cortical bone. The main limitations of this study were the limited number of samples and the potential variations between the rib bone samples. These results might not be applicable to clinical situations. Bone cement should become resorbed and replaced by newly formed bone if allowed the proper amount of time. Further studies are necessary to confirm the clinical performance of bone cement grafts in in vivo animal studies.




 XML Download
XML Download