

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Several systemic diseases exhibit oral and gingival manifestations, and thus dentists can play an important role in the early diagnosis of these diseases. Granulomatosis with polyangiitis (GPA), formerly known as Wegener's granulomatosis, is one such disease that may have gingival manifestations. GPA is a potentially life-threatening disease characterized by necrotizing granulomatous inflammation and small vessel vasculitis. The precise etiology of GPA remains unknown. It chiefly affects the upper and lower respiratory tract and kidneys, but can affect any part of the body or any of its organs [123]. Inflammation of the blood vessels leads to damage to vital organs. Without treatment GPA usually runs a rapid and fatal course with most patients not surviving more than a year after diagnosis [456].
Oral involvement of GPA has been observed in approximately 6%–13% of patients [7] and its manifestation includes oral mucosal ulcerations and nodules. However the most characteristic oral lesion is hyperplastic gingivitis presenting with a “strawberry like” appearance [5,8]. Occasionally oral lesions are observed before multi-organ involvement occurs. The diagnosis of GPA is made based on clinical symptoms and signs, the presence of the anti-neutrophil cytoplasmic antibody (ANCA), and a positive biopsy [9]. Because of its rapid progression and potentially fatal outcome, an early diagnosis is important. Therefore, knowledge and information about lesions that are considered strongly indicative of GPA would be valuable for facilitating diagnosis.
This report describes a case of GPA with orofacial features including a gingival manifestation. The observation of the gingival manifestation led us to suspect and make an early diagnosis of GPA, allowing rapid treatment to be initiated. In this report we also describe a review of the current literature with a focus on current knowledge of the disease characteristics, the criteria for diagnosis, and the treatment options.
CASE DESCRIPTION
A 57–year-old sailor presented to the Department of Dentistry at Ulsan University Hospital complaining of gingival swelling since approximately 2 months that had worsened over the preceding 2 weeks. He had also observed multiple skin ulcers on his face; these symptoms had prompted him to visit the Department of Dermatology at our hospital immediately prior to his visit to our department. He stated that the facial and oral lesions had appeared almost simultaneously. Because he was a sailor, he had not been able to seek proper treatment before leaving his ship. His medical history was otherwise unremarkable.
Upon clinical examination, he had swollen erythematous gingivae with petechiae that had the appearance of the surface of a strawberry. Besides the facial skin ulceration and gingival lesions the examination revealed nothing remarkable (Figure 1). Panoramic radiographs revealed no evidence of any underlying bone involvement although multiple teeth mobility was observed. Laboratory results revealed a C-reactive protein concentration of 0.72 mg/dL and an erythrocyte sedimentation rate of 28 mm/hr but no leucocytosis (7,390/µL). A human immunodeficiency virus test was negative, renal function and urinary sediment tests were normal, and all other results were unremarkable.
Figure 1
An image showing the granulomatous ulcerations on the patients’ face and the “strawberry-like”appearance of the upper/lower gingivae.

The initial differential diagnosis included pyogenic granuloma (PG) and GPA. Because a “strawberry-like” gingivitis has been suggested to be a characteristic sign of GPA, the patient was advised to undergo an incisional biopsy of the affected gingiva. The patient was immediately started on a course of antibiotics whilst the histopathology results were awaited. The patient failed to show any signs of recovery as a result of the antibiotic treatment. On a return visit to the hospital one week later, the patients’ signs and symptoms had worsened with partial bony exposure of the maxillary anterior alveolar portion evident (Figure 2).

The histopathologic examination of the biopsied tissue showed chronic active inflammation with abscess, fibrinoid vasculitis and granulation of the tissue (Figure 3). Based on these findings, and the clinical presentation of strawberry gingivitis and facial lesions, a diagnosis of GPA was strongly suspected and it was decided to analyze blood levels of ANCA. Laboratory testing demonstrated a positive cytoplasmic anti-neutrophil cytoplasmic antibody (c-ANCA) result and an associated increase in proteinase 3 ANCA (PR3-ANCA) levels suggesting a diagnosis of GPA.
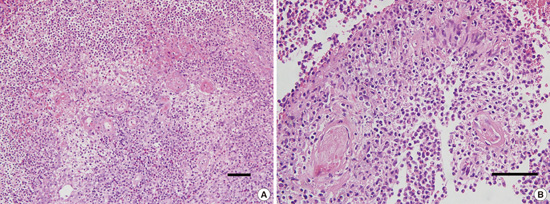
Figure 3
Histopathologic features of the affected upper anterior gingiva. (A) A diffuse mixed inflammatory cell infiltrate comprising mostly neutrophils that formed micro-abscesses. Also evident is the presence of fibrinoid vasculitis. (B) This image shows palisading granulomas and fibrinoid vasculitis. (A, B: H&E staining)

We referred the patient to the Department of Internal Medicine, for further evaluation and a systemic work-up, where the diagnosis of GPA was confirmed. Chest radiography and CT imaging of the sinuses was normal. The patient was admitted and started on a disease-modifying therapy regimen, which included 12.5 mg of methotrexate a day, once every 7 days, and 40 mg of prednisone daily. He was followed up by the rheumatologists and us. After 10 days of treatment, improvement in the patient was observed (Figure 4), and he was discharged from the hospital on day 14. As the oral hygiene and periodontal status of the patient had worsened due to the gingival swelling, we advised him on good oral hygiene and performed scaling on the day of discharge. Two months after initiation of the treatment, prednisone was progressively tapered to 2.5 mg for maintenance; the facial and gingival lesions did not show signs of relapse.

DISCUSSION
Several systemic diseases exhibit characteristic oral manifestations, which dentists can identify or diagnose. Some of these systemic conditions, including sarcoidosis, inflammatory bowel disease (IBD), Melkersson–Rosenthal syndrome (MRS), and GPA, can show oral granulomatous lesions [10].
GPA was first described as a separate entity from peri-arteritis nodosa by Friedrich Wegener in 1937 and was formerly known as Wegener's granulomatosis. It is a form of primary systemic vasculitis characterized by granulomatous inflammation of the soft tissue as well as fibrinoid vasculitis of the small to medium sized vessels of the body [123,11,12]. The precise etiology remains unknown, although microbes such as bacteria and viruses as well as genetic factors have been implicated in its pathogenesis [13].
The reported annual incidence of GPA varies from 2–12 per million and its prevalence is estimated to be 24–157 per million [3]. Although the age of the patient at diagnosis is generally 45–60 years, it can present at any age [3,14]. The incidence of GPA is equal in men and women, and it is more common in Caucasians than in other ethnic groups [15].
GPA can be classified clinically as localized, early systemic, or generalized [5,15]. Localized forms of GPA predominantly affect the upper respiratory tract, whereas generalized forms can show various combinations of renal manifestations, alveolar hemorrhage, and vital organ involvement with altered general condition [3,16].
The incidence of oral manifestations in GPA range from 6%–13% of patients, and the mouth is the initial site of clinical presentation in 5%–6% of cases [5,7]. Oral manifestations of GPA include mucosal ulceration that can affect the buccal or lingual mucosa, mouth floor, posterior pharynx and tonsils, and labial mucosal nodules [17]. Upper anterior gingivae are usual oral site of involvement of GPA; the affected gingivae may be red to purple in color and have petechiae that resemble an “over-ripe strawberry” [2,4,5]. The “strawberry-like” appearance of the gingivitis has been suggested to be a particularly characteristic sign of GPA. Osteomyelitis or necrosis of the underlying bone can develop with subsequent mobility and loss of teeth [18]. Oral lesions can remain localized for unusually long periods of time before multi-organ involvement occurs [19].
The American College of Rheumatology criteria for the classification of GPA are as follows: abnormal urinary sediment (the presence of red cell casts or greater than five red blood cells per high power field), abnormal findings on chest radiograph (nodules, cavities, or fixed infiltrates), oral ulcers or nasal discharge, and granulomatous inflammation on biopsy. For the diagnosis of GPA, a patient must have at least two of these four criteria [4,19,20]. The presence of any two or more criteria gives a sensitivity of 88.2% and a specificity of 92.0% [16]. These tests in combination with biopsies were used before the discovery of ANCA and have greatly facilitated the diagnosis of GPA. The presence of ANCA is the most important serological test in the diagnosis of vasculitis. In patients with GPA, a positive ANCA result with a cytoplasmic distribution that binds to PR3-ANCA using an enzyme-linked immunosorbent assay is a typical finding. ANCA serology has a sensitivity of 90% and a specificity of 96% in detecting GPA [3,21,22]. Therefore, a combination of clinical presentation, biopsy, and a positive c-ANCA result provides the most effective approach for diagnosis.
Delay in the diagnosis of GPA is unfortunately common and this often leads to serious morbidity or even fatal outcomes. Left untreated, only 18% of GPA patients survive beyond one year [23], with renal failure being the most common cause of death. The aim of treatment is twofold: to target the outward signs of the disease in order to improve the patient's symptoms, and to prevent the onset of severe renal disease. It has been suggested that the choice of therapeutic agents for the treatment of GPA should depend on the severity of the disease and whether the signs are localized or generalized [24]. In recent times mortality due to GPA has been significantly reduced by the use of cytotoxic therapy with cyclophosphamide and glucocorticoids [15]. After the introduction of cytotoxic drugs in combination with steroids, the 5-year survival rate has been reported to be over 75% [25]. Although the recommended treatment consists initially of high doses of steroids in combination with immunosuppressive therapy using cyclophosphamide, long-term treatment with cyclophosphamide has been associated with an increased incidence of severe side effects such as hemorrhagic cystitis, bladder cancer, lymphoma, and bone marrow suppression [5,15,16,26]. Therefore, methotrexate or azathioprine have been suggested as a substituted for cyclophosphamide [15,16]. In the present case methotrexate was used instead of cyclophosphamide. Although some lesions respond well to treatment, relapse and acute renal failure can occur within months [27]. Thus, frequent follow-up examinations are required to ensure adequate control of the disease.
The patient in this case report had orofacial granulomatous lesions. Facial granulomatosis is an important element in the differential diagnosis of other granulomatous diseases, such as tuberculosis, systemic fungal infections, leprosy, and foreign body reactions [28]. Hence, these pathologies can also be suspected when patients present with only the facial lesions. In fact, our patient’s dermatologist suspected tuberculosis or other infection based purely on the physical examination of the face. However, they were later ruled out based on the patient’s medical history, general and systemic examination, and the laboratory results. Patients with sarcoidosis, IBD, and MRS can also present with similar orofacial granulomatous lesions, and these diseases should be ruled out. The skin lesions of sarcoidosis usually resolve spontaneously in 2–4 weeks, but our patient’s lesions had worsened over 2 months. Moreover, he did not have abdominal pain, diarrhea, and rectal bleeding commonly associated with IBD, and recurring facial paralysis and swelling associated with MRS. Although PG commonly manifests as lesions on the skin or in the oral cavity and the gingiva, they rarely exceed 2.5 cm in size [29]. Moreover, because a “strawberry-like” gingivitis is a characteristic sign of GPA, we suspected GPA based on his clinical presentation and histology. Hence, we decided to perform the ANCA test that revealed a positive c-ANCA titer and associated PR3-ANCA levels coinciding with the diagnosis of GPA. The gingival manifestations of the disease were crucial in the diagnosis.
In conclusion, this patient presented with orofacial granulomatous lesions. Because of the presentation, we believe we were better able to identify GPA as a potential diagnosis than a dermatologist who, based purely on an examination of the patient's face, would be more likely to have suspected tuberculosis or another infection. The specific gingival manifestation of strawberry gingivitis permitted an early diagnosis and prompt therapy in a disease where time is a crucial factor. The present case report highlights the critical role dentists can play in the diagnosis and even management of GPA. Because failure to recognize the diagnostic clinical picture may result in a potentially lethal delay in deciding on an appropriate treatment strategy for this disease, dentists should be aware of the oral signs and symptoms of systemic diseases such as GPA.
 XML Download
XML Download