

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
After the concept of osseointegration was introduced by Brånemark et al. [1], the indications for dental implants were expanded from fully edentulous to partially edentulous cases and a high long-term success/survival rate was demonstrated [2,3]. Despite the general reliability of implantation techniques, it is not always possible to perform a restoration without any complications. In the literature, the complications arising from implants have been categorized into two types: technical and biological [4,5,6,7,8,9]. The general category of technical complications refers to any mechanical damage of the implants, implant components, and suprastructures, whereas biological complications are disturbances in implant function that affect the supporting peri-implant tissues [8]. According to previous studies [4,5,6,7,9], the overall survival rate of implants ranges from 94.5% to 97.2%. However, the incidence of biological and technical complications has varied widely as implant systems have changed over time.
Implant systems can generally be classified as either external connection systems (ECSs) or internal connection systems (ICSs) according to the type of fixture or abutment connection. ICS can be subdivided into bone-level systems (ICS-BL) and transmucosal systems. ECSs are characterized by an external hexagon and have served well over the years. The external hexagon was developed to facilitate the insertion of components such as abutments and impression copings, rather than to provide an antirotational ability [6] and therefore, external systems exhibit weakness due to micromovements of the abutments under a high occlusal load due to their limited hexagonal height [5]. ICSs typically have a tapered conical connection and are popular for their mechanically stable and self-locking interface [9]. It has been shown that the conical internal connection transfers stress from the abutment apically to a greater extent and, as a result, reduces stress on the crestal bone in comparison with external connections [10]. However, fractures may occur in the coronal portion of some ICS-BL fixtures under a high occlusal load [11].
Abundant long-term clinical data regarding ECSs are available. Most technical complications are well-reported, and it is known that the fixtures in ECSs can experience breakage of the abutment screw instead of undergoing fixture fracture, with potentially catastrophic results [10,12]. In contrast, few long-term clinical data have been reported for ICSs, and the mechanical advantages of ICSs have been assessed based on in vitro studies. Moreover, recent studies have challenged the mechanical stability of ICSs and have shown that increased axial displacement occurs in ICSs as tightening torque and loading cycles increase [13,14,15].
Although abundant studies have investigated survival rates and/or complication incidences, no comparative studies of different implant/abutment connection systems have been performed. As a consequence, survival rates and the incidence of complications according to the type of implant/abutment connection can only be indirectly compared in systematic reviews [4,16]. Therefore, the present study was conducted to retrospectively compare the survival rates and the incidence of post-loading complications in two implant systems-one an ICS-BL and the other an ECS-installed in one institution.
MATERIALS AND METHODS
This study was a retrospective analysis of the cumulative survival rates (CSRs) and the incidence of complications in two implant systems-one ICS-BL (ASTRA Tech Implant System EV, Dentsply Implants, Mölndal, Sweden) and one ECS (Brånemark Implant System, Nobel Biocare, Göteborg, Sweden)-and was approved by the Institutional Review Board at Asan Medical Center (S2012-2211-0001). A total of 2,651 implants in 1,074 patients were reviewed, including all types of implant prostheses, such as fixed partial or full-arch restorations, hybrid-type restorations and overdentures. All the patients were treated in the Department of Dentistry, Asan Medical Center in Seoul, South Korea between January 2007 and December 2010.
A thorough and complete review of the medical records of the enrolled patients was performed and all data were inserted into spreadsheets (Microsoft Excel 2007, Microsoft Inc., Redmond, WA, USA). The collected data included the implant system (ASTRA Tech or Brånemark), the position of the fixture, the diameter and length of the fixture, the date of fixture installation, the date of prosthesis delivery, the date of the last visit, the type of prosthesis (fixed partial, fixed full-arch, hybrid, or overdenture), the type of crown retention (screw, cement, or screw-cement), the type of superstructure (gold, metal-ceramic, or all ceramic), the date of fixture removal due to failure (if any), the probing depth around the implant crown, thread exposure in follow-up radiographic images taken after at least three months of loading, soft tissue complications, chipping of the veneering material, fracture of the implant, fracture of the implant crown, loosening or fracture of the abutment or screw, loss of retention, and loss of access hole filling material. Thread exposure in radiographic images was defined as marginal bone loss involving more than two threads exposed in an ECS or extending beyond the microthread region in an ICS-BL [4,17]. A soft tissue complication was considered to be present if records indicated signs of inflammation, bleeding on probing, suppuration, hyperplasia, or dehiscence in the peri-implant mucosa. Among the complications recorded, probing pocket depth>4 mm, thread exposure in follow-up radiographic images, and soft tissue complications were considered to be biological complications, whereas chipping of the veneering material, fracture of the implant, fracture of the implant crown, loosening or fracture of the abutment or screw, loss of retention, and loss of access hole filling material were considered to be technical complications.
The observation period of an implant was defined as the time interval from the day of prosthesis delivery to the day of the last visit in a patient's medical record. Survival was defined as the condition of an implant remaining in situ with or without modifications, while failure was defined as the condition of an implant that had to be removed [18]. CSRs were calculated using time-table survival probabilities and the log-rank chi-square test was used to compare the survival rates between the two implant systems. The incidence of biological and technical complications between the two systems was compared with the Pearson chi-square test. The statistical analysis was carried out with IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA), and P-values <0.05 were considered to indicate statistical significance.
RESULTS
The characteristics of the subjects according to the type of implant that was placed are presented in Tables 1 and 2. A total of 1,074 patients aged between 14 and 92 years (mean, 53.1±13.5 years) at the time of fixture installation, of whom 484 were female, were enrolled in the study. A total of 2,651 implants (1,167 ICS-BLs and 1,484 ECSs) were placed in the 1,074 patients (551 ICS-BLs and 523 ECSs), with an approximate average of 2.47 implants per patient. A total of 653 ICS-BL implants (56.0%) and 727 ECS implants (49.0%) were inserted in the maxillae, while 659 ICS-BL implants (56.5%) and 836 ECS implants (56.3%) were placed in the molar region. The average observation periods for the ICS-BL and ECS were 3.4 years (range, 0.1-6.2 years) and 3.1 years (range, 0.1-6.0 years), respectively. More than half of the superstructures were fixed partial prostheses of screw-retained gold crowns with resin veneering.
Cumulative survival rate
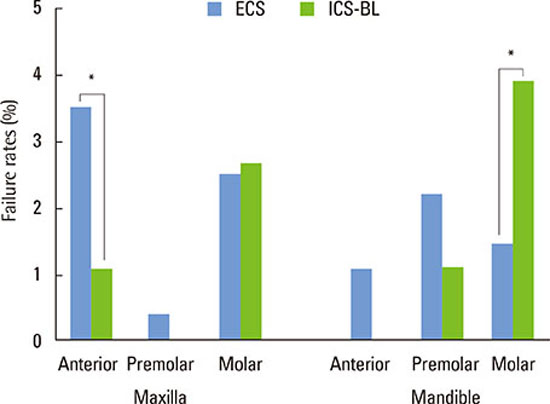
The overall CSR after six years was 96.1%. No statistically significant difference between the two systems was observed, although the CSR for the ICS-BL (94.9%) was lower than that for the ECS (97.1%) (Table 3). Both systems showed similar pattern of failure occurrence, in which more than half of failures occurred in the first year of loading. The ICS-BLs mostly failed in the molar region, whereas the failure rate of the ECSs did not significantly vary depending on the position of the implant. Moreover, higher failure rates were observed in the ICS-BLs in the mandibular molar region and in the ECSs in the maxillary anterior region (P<0.05) (Fig. 1).
Complication incidence
Fig. 2 shows the incidence of complications in the two implant systems. Biological complications (2.1%-10.4%) were more frequent than technical complications (0.1%-6.9%). Of all the complications investigated, soft tissue complications had the highest incidence (8.1% in the ICS-BLs and 10.4% in the ECSs), followed by loosening or fracture of the abutment or screw (6.9% and 3.2%, respectively), probing pocket depth>4 mm (4.0% and 4.3%, respectively), and chipping of the veneering material (3.5% and 3.0%, respectively), while the incidence of other complications was less than 3.0%. Fractures of the implant or crown occurred very rarely. Regardless of statistical significance, the ECSs tended to show more biological complications while the ICS-BLs were more prone to technical complication. Moreover, soft tissue complications were more frequent in the ECSs (P=0.005) and loosening or fracture of the abutment or screw occurred more frequently in the ICS-BLs (P<0.001).
DISCUSSION
The present study compared the CSRs and the incidence of complications in two different implant systems. Since most commercially available implant systems yield a satisfactory outcome in terms of osseointegration, postloading complications are of primary importance for the long-term success of an implant. In order to ensure the usefulness of our data in future systematic reviews or meta-analyses, the functional complications of implants were categorized according to Misch and Wang's criteria [8]. Previous studies of implant complications have either involved one system with a small number of subjects or several systems with a relatively large number of subjects. Analyses of one system with a small number of subjects may present in-depth information on the system studied, but are not more generally relevant due to their small sample sizes. Meanwhile, the extant studies on several systems with a large number of subjects were conducted using a multicenter design, in which the collected data are often heterogeneous. In the present study, more than 500 subjects with more than 1,000 implants for each system were enrolled, and all procedures were performed in the same center. These considerations increase the relevance of the present study.
The six-year CSRs were 94.9% for the ICS-BL and 97.1% for the ECS. These CSRs correspond to those reported in previous studies [4,19]. Although ECSs had a higher CSR than ICS-BLs, the difference was not statistically significant. This result should be interpreted with caution because the incidence of failure of the ICS-BLs was higher through the second year to the sixth year compared to that of the ECSs. The more frequent failure in the ICS-BLs was partly associated with fractures of the fixture. Previous studies have shown an incidence of fracture of 0.7% for ICS-BLs and 0.18% for ECSs [20,21]. Cha et al. [11] also reported that 11 of 136 implants were removed due to implant fracture within five years. For a proper and accurate comparison of the two systems, long-term CSRs of more than 10 years should be examined.
Previous studies comparing these two systems focused on technical complications [4,22] and no studies have compared biological complications in these systems. In the present study, both categories of complications were simultaneously investigated and compared. Soft tissue complications, which fall into the category of biological complications, were the most frequent complication. However, it is possible that the incidence of soft tissue complications was underestimated, since bleeding on probing or soft tissue enlargement/dehiscence around the implant can often be observed in daily practice. Unfortunately, no previous studies have evaluated the incidence of soft tissue complications. The second most frequent complication was loosening or fracture of the abutment or screw, which falls into the category of technical complications. Loosening or fracture of the abutment or screw also included a broad range of situations, which may contribute to its high incidence. Other studies have reported a 5% and 9% occurrence of screw loosening [20,23], which are comparable to our results. It was noteworthy that soft tissue complications were more frequent in the ECS and loosening or fracture of the abutment or screw occurred more frequently in the ICS-BL. Moreover, regardless of statistical significance, the ECS tended to show higher incidences of biological complications, while the ICS-BL was more prone to technical complications.
Recent systematic reviews have reported that the cumulative complication rate of >2 mm of bone loss in implants was 5.2% [20], and two other systemic reviews have shown marginal bone loss rates of 2.6% and 5.7% [21,23]. In the present study, thread exposure in radiographs was used as a parameter indicating marginal bone loss and had an incidence of 2.1% and 2.5% for the ICS-BLs and ECSs, respectively. The low incidence compared to those found in the previous reviews may reflect the loose definition of thread exposure in radiographs. However, the loose definition was sufficient to compare the incidences between the two systems because the dimensions of the microthread region in the ICS-BL were similar to those from the platform to the second thread in the ECS.
The higher incidence of soft tissue complications in the ECSs could partly be explained by the effect of platform-switching [24], which was employed in the ICS-BL. In platform-switched systems, some additional thickness in the horizontal soft tissue component might contribute to reducing crestal bone loss resulting from the reformation of biologic width and the microgap. However, another comparative study between platform-matching and platform-switching systems showed minimal marginal bone-level changes with no difference between the implant systems [25]. Taking these studies into account, we suggest that soft tissue complications such as signs of inflammation, bleeding on probing, and suppuration on peri-implant mucosa may be associated with the stability of peri-implant soft tissues rather than that of peri-implant marginal bone level, and that the ICS-BL can stabilize adjacent soft tissues more than the ECS can. However, further studies are required because other factors, including the emergence profile of the crown and the location of the crown margin in a cement-retained crown, can affect the condition of peri-implant soft tissue.
The frequency of loosening or fracture of the abutment or screw has been reported to be 12% and 19% [17,20], but was much lower in the present study (6.9% in the ICS-BLs and 3.2% in the ECSs). The relatively short follow-up period and the use of a single implant system for each connection type may play a role in these low complication rates. Moreover, in the present study, loosening or fracture of the abutment or screw occurred more often in the ICS-BLs. No previous study has directly compared the occurrence of this complication between the two systems. In recent publications, conflicting results have been reported: more screw loosening has been observed in ECSs, while more axial displacement and a decrease of loosening torque have been reported in ICS-BLs [15,16,26]. Another study conducted in our institution also reported a 25.7% rate of abutment screw loosening in single ICS-BL implant restorations up to five years [11]. Maeda et al. [10] demonstrated that the thinner lateral wall at the coronal part of an ICS fixture was related to fixture tearing or fracture. Furthermore, the ICS-BLs showed a faster CSR decrease than did the ECSs over time, which may be another indication that the coronal portion of fixtures in the ICS-BL is relatively weak.
In conclusion, within the limitations of this retrospective study, the ICS-BLs were more prone to technical complications while the ECSs were more vulnerable to biological complications. For this reason, the ICS-BL may be more suitable for restoring anterior regions experiencing esthetic challenges, whereas the ECS may be preferred in posterior regions under a high occlusal load.




 XML Download
XML Download