

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Guided bone regeneration (GBR) has become an indispensable technique for enhancing new bone formation around peri-implant dehiscence defects [12]. Non-cross-linked native collagen membrane (NCM) is the most widely used type of membrane in the GBR technique. It shows excellent biocompatibility with a low immune response, and has the advantage of promoting wound healing by inducing fibroblast migration [345]. In addition, the bone regeneration capacity of NCM is similar to that of nonresorbable membrane [6]. Despite these advantages, the shortened functional period due to a loss of cell occlusiveness and greater susceptibility to degradation by periodontal bacteria may restrict bone regeneration when using NCM [78].
Various cross-linking methods have been investigated and developed with the aim of improving the mechanical properties and compensating for the disadvantages of NCM [9]. Chemical and physical modifications are important for increasing the degree of cross-linking between collagen fibers, which varies significantly with the cross-linking method used [10]. However, all cross-linked membranes reportedly increase thermal stability, mechanical strength, and resistance to enzyme activity [11].
Chemically cross-linked collagen membrane reportedly exhibits biocompatibility with a minimal inflammatory response and has been used for GBR; however, several randomized controlled clinical studies have also demonstrated that it exerts significant adverse effects on bone regeneration [12131415]. For example, Becker et al. [14] reported that while chemically cross-linked collagen membrane provides predictable bone augmentation, it is also frequently associated with premature membrane exposure and wound infections. In addition, Annen et al. [15] showed that chemically cross-linked collagen membrane with an extended resorption time was associated with significantly more complications and a lower bone regeneration efficacy compared to NCM.
Dehydrothermal (DHT) treatment is a major physical modification method used in the production of a cross-linking collagen matrix. In vitro studies have demonstrated that DHT cross-linked collagen membrane (DCM) exhibits a high tensile strength and resistance to degradation, and reduced cytotoxic responses [1617]. Rothamel et al. [18] showed that DCM and NCM have similar biocompatibility in rabbits, and that DCM provides an adequate environment for bone remodeling with sufficient vascularization during the initial healing phase as well as long-term structural stability. However, despite these positive results in animal studies, few clinical and controlled human studies have assessed the efficacy and safety of DCM.
The aim of this study was to determine the clinical feasibility of DCM for use in bone regeneration around peri-implant dehiscence defects, and compare it with that of NCM.
MATERIALS AND METHODS
Study design
A randomized, single-blinded, single-center clinical trial was conducted to evaluate the clinical feasibility and bone regeneration capacity around peri-implant dehiscence defects of two types of membrane. The study was approved by the Institutional Review Board (IRB) for Clinical Research at Dental Hospital of Yonsei University (approval no. 2-2013-0021). All patients provided written fully informed consent in accordance with IRB guidelines for enrollment, and the study was conducted in accordance with the Declaration of Helsinki and the Guidelines on Good Clinical Practice [19].
Study population
A total of 43 patients who needed single-tooth implant treatment from August 2013 to October 2014 were included in this clinical study. The following inclusion criteria were applied: (1) male or female aged ≥20 years, (2) healthy systemic condition (including well-controlled medical illnesses), (3) a vertical dehiscence defect (only on the buccal side) of ≥3 mm present immediately after implant placement, (4) secure primary stability of the implant, and (5) no allergic reaction to collagen. The following exclusion criteria were applied: (1) severe or uncontrolled systemic disease, (2) advanced or untreated periodontitis, (3) pregnancy or breastfeeding, (4) history of radiation therapy to the head or neck, (5) hormones or bisphosphonate therapy affecting bone or connective tissue metabolism, and (6) heavy smoking (>20 cigarettes/day).
Sample size calculation
The required sample size was determined using the two-sided t-test at an alpha level of 0.05 and a statistical power of 80%. The threshold for differences in bone regeneration capacity between the NCM and DCM groups was set to 1.0 mm, and the standard deviation was assumed to be the same for both groups according to the results of a previous study [2021]. These parameters resulted in a required sample size of 28 patients, and so 30 patients were enrolled (15 patients in each group) to account for a potential dropout rate of 10%. The statistical power was calculated using G* Power 3.1 (University of Duesseldorf, Germany) [22].
Randomization
Randomization took place after implant placement using online databases for clinical trials (Sealed Envelope™, sealedenvelope.com). The 30 enrolled patients were assigned to either the NCM group (n=15) or the DCM group (n=15) according to computer-generated random numbers. None of the patients knew whether they received the control or experimental membrane until after the end of the study.
Surgical procedures
All steps in the surgical procedures and all evaluation parameters were calibrated in training and calibration sessions. All patients received antibiotics (amoxicillin 500 mg or roxithromycin 150mg daily), a single dose of analgesic (ibuprofen 200mg), and mouthwash (GUM Activital, Sunstar, Osaka, Japan) after implant surgery for 7 days. Full-thickness flaps were elevated, with vertical incisions made when necessary. A surgical stent was prepared for the optimal implant position, and a sandblasted, large-grit,acid-etched (SLA) surface internal-type implant fixture was placed in accordance with the manufacturer’s recommended protocol. A sealed randomization envelope was opened to allocate augmentation of the defect, with either porcine dermis-derived non-cross-linked type I and III collagen (BioGide® Geistlich Biomaterials, Wolhusen, Switzerland) or porcine pericardium-derived type I collagen membrane (OssGuide®, Bioland, Cheongju, Korea) and xenograft bone substitutes (BioOss®, Geistlich Biomaterials, Wolhusen, Switzerland, and CollaOss®, Bioland, Cheongju, Korea). After implant placement in the ideal prosthetic position, the horizontal and vertical dehiscence defect was augmented. A collagen membrane was trimmed so that it extended 2–3 mm from the defect margin. Flaps were sutured with 6-0 absorbable sutures (Monosyn 6–0, B. Braun Aesculap, Tuttlingen, Germany), with a horizontal periosteal releasing incision used where necessary to attain primary and tension-free closure of the flap. Follow-up was performed three times during 8 weeks and additional care was arranged according to the needs of individual patients.
Clinical analysis
All horizontal and vertical defects were measured using a 15-mm UNC periodontal probe (CP 15 UNC, Hu-freidy, Chicago, IL, USA) at the time of implant installation and re-entry surgery. The same trained and calibrated examiners carried out all measurements. The following parameters were measured: (1) defect width (DW), measured as the linear distance between the widest points on the medial and distal sides of the buccal aspect; (2) defect height (DH), measured as the linear distance from the top of the implant platform to the initial bone-to-implant contact at the buccal aspect; (3) a change in the defect width (ΔDW), calculated as DW (re-entry surgery) – DW (baseline); and (4) a change in the defect height (ΔDH), calculated as DH (re-entry surgery) – DH (baseline).
The ease of manipulating and maintaining NCM and DCM in implant surgery was clinically assessed using scores on a visual analog scale (VAS) that ranged from 0 (very good) to 10 (very poor). The following parameters were measured: (1) manipulation of the membrane, degree of hydrophilicity and handling during the GBR procedure; and (2) maintenance of augmented bone substitutes, and whether covering the membrane after augmentation with bone materials improved the stability.
Radiographic analysis
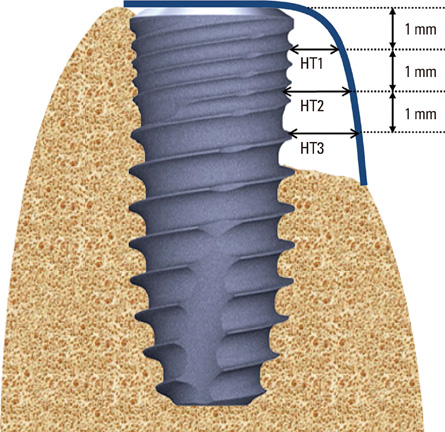
Cone-beam computed tomography (CBCT; Alphard Vega, Asahi Roentgen, Kyoto, Japan) was performed to assess the horizontal thickness (HT) immediately after augmentation and at the time of re-entry surgery. The following parameters were measured (Figure 1): (1) horizontal thickness of horizontal augmented bone located 1, 2, and 3 mm below the top of the implant platform (HT1, HT2, and HT3); (2) changes in horizontal thickness at each level, calculated as HT (re-entry surgery) – HT (baseline) (ΔHT1, ΔHT2, and ΔHT3); (3) density of the newly formed bone located 1 mm below the top of the implant platform, assessed using the Hounsfield unit (HU) scale with computed-tomography image-processing software (OnDemand3D®, CyberMed, Seoul, Korea) (bone density of HT1).
Histological analysis
After a healing period of 16 weeks, when there was sufficient keratinized tissue around the top of the implant cover screw, a thin strip-shaped soft-tissue biopsy sample was obtained prior to performing re-entry surgery and the connection of the abutment. The biopsy samples were fixed in 10% neutral formalin for 10 days, and then trimmed and dehydrated in a graded series of alcohol solutions. All specimens were stained with hematoxylin-eosin and Masson’s trichrome stains. The slides were observed under a light microscope (BX50, Olympus, Tokyo, Japan).
Research protocol alteration
During concurrent research that is currently still in progress, we determined that the use of different bone substitutes in the NCM and DCM groups interfered with evaluations of membrane efficiency. Therefore, after obtaining re-approval from the IRB, we used the same bone graft materials (BioOss®) in both groups, and altered the study to focus on the clinical feasibility of the membrane.
Statistical analysis
The mean±standard deviation values and 95% confidence intervals were estimated for each study group. Statistical analyses were performed with IBM SPSS Statistics (Version 21.0, IBM Corp, Armonk, NY, USA), using independent t-tests to compare the results between the NCM and DCM groups (P<0.05).
RESULTS
Patient enrollment
The 30 enrolled patients who fulfilled the inclusion and exclusion criteria comprised 16 males and 14 females with a mean age of 53.3 years (range, 31 to 75 years). Two patients dropped out during the follow-up: one patient in the DCM group showed signs of local infection such as gingival swelling, redness, and pus discharge at the 4-week checkup, and so the implant fixture was removed; the other patient was in the NCM group and showed early exposure of the cover screw at the 8-week checkup, and so an emergency surgical procedure involving healing around the abutment connection was performed (Figure 2). The remaining 28 patients (mean age, 53.4 years; range, 31 to 75 years) experienced no critical adverse events (Table 1).
Figure 2
Flow chart of patient enrollment and reasons for exclusion. NCM: non-cross-linked native collagen membrane; DCM: dehydrothermally cross-linked collagen membrane; CBCT: cone-beam computed tomography.

Table 1
Characteristics of enrolled patients in the two study groups.
| Characteristic | NCM group | DCM group | Total |
|---|---|---|---|
| Sample size | 14 | 14 | 28 |
| Gender | |||
| Male | 9 | 5 | 14 |
| Female | 5 | 9 | 14 |
| Age | |||
| Mean age (years) | 52.1 | 54.6 | 53.3 |
| Age range (years) | 31-71 | 41-75 | 31-75 |
The implants were distributed as follows: incisor, n=10 (35.7%); bicuspid, n=7 (25%); and molar, n=11 (39.3%). The 30 implants investigated in these patients comprised the following 4 models, all of which had an internal-connection design: Implantium and NR line® (Dentium), n=22 (78.6%); TS III® (Osstem), n=2 (7.1%); Bone Level® (Straumann), n=3 (10.7%); and Luna® (Shinhung), n=1 (3.6%). The diameter of the most commonly used implant was 4.8 mm (n=8, 28.6%), while the other implants had the following diameters: 3.8 mm (n=8, 28.6%), 4.3 mm (n=5, 17.9%), 3.3 mm (n=2, 7.1%), and 3.6, 4.1, 4.5, 5.0, and 6.0 mm (n=1 each, 17.9%). The implants had the following lengths: 10 mm (n=19, 67.9%), 8 mm (n=5, 17.9%), 12 mm (n=2, 7.1%), and 8.5 and 9 mm (n=1 for each, 7.1%, Table 2).
Table 2
Characteristics of implants.

Clinical findings
In the present study we attempted to determine the clinical feasibility of using DCM compared with NCM for treating human peri-implant dehiscence defects. We therefore conducted experiments that excluded bone graft materials from the evaluations, and assessed only the membranes themselves.
Five defect sites (two sites in the NCM group and three sites in the DCM group) showed soft-tissue dehiscence defects and membrane exposure during the early healing period. Despite the presence of plaque accumulation and signs of mild inflammation around the soft-tissue dehiscence defects, additional necrosis and secondary dehiscence defects did not occur. Spontaneous secondary closures were successfully completed, and no significant differences were observed between the two groups at the 8-week follow-up.
The DW value decreased from 3.8±1.3 to 0.4±0.9 mm in the NCM group and from 3.5±1.1 to 1.7±1.6 mm in the DCM group; the corresponding ΔDW values were 3.5±1.2 and 1.7±2.2 mm, respectively. Similarly, the DH value decreased from 5.1±2.4 to 0.2±0.6 mm in the NCM group and from 4.5±2.2 to 1.1±1.2 mm in the DCM group, with corresponding ΔDH values of 5.0±2.5 and 2.9±2.3 mm, respectively. The ΔDW and ΔDH values were statistically significant between groups (P=0.016 and P=0.031, respectively; Table 3).
Table 3
Clinical measurements of horizontal and vertical dehiscence defects.

Data are mean±SD values.
NCM: non-cross-linked native collagen membrane, DCM: dehydrothermally cross-linked collagen membrane, DW: defect width, DH: defect height, ΔDW: DW (re-entry surgery) – DW (baseline), ΔDH: DH (re-entry surgery) – DH (baseline).
a)Statistically significant difference in clinical measurements between the two groups (P<0.05).
The clinical assessment of the ease of manipulation and maintenance was based on the VAS scores in the two groups. The VAS score for membrane manipulation did not differ significantly between the NCM group (0.5±1.0; range, 0 to 3) and the DCM group (1.3±1.7; range, 0 to 5; P=0.119). In contrast, the VAS score for the maintenance of augmented bone substitutes did differ significantly between the two groups: 0.3±0.7 (range, 0 to 2) in the NCM group and 1.3±1.1 (range, 0 to 3) in the DCM group (P=0.012, Table 4).

Radiographic findings
The mean HT and corresponding ΔHT values were comparable in the two groups (Table 5). The HT values decreased and the corresponding ΔHT values increased by similar amounts in the two groups, and there were no statistically significant differences among any of the ΔHT values (Table 4).
Table 5
Measurements made in the radiographic analyses.
Data are mean±SD values.
HT1, HT2, and HT3: horizontal thicknesses at 1, 2, and 3 mm below the top of the implant platform, ΔHTx: HTx (re-entry surgery) – HTx (baseline), NCM: non-cross-linked native collagen membrane, DCM: dehydrothermally cross-linked collagen membrane.
a)Statistically significant difference between the two groups in radiographic measurements (P<0.05).
The bone density of HT1 as assessed at the time of re-entry surgery did not differ significantly between the NCM group (769.5±218.2 HU; range, 421.1 to 1163.7 HU) and the DCM group (739.6±275.1 HU; range, 280.4 to 1179.4 HU; P=0.752).
Histological findings
There was insufficient keratinized gingiva around the implant in six patients, and so histological slides from the remaining 10 DCM and 12 NCM specimens were examined by light microscopy. Soft tissue biopsy was performed to confirm the presence of the remaining membrane fragment. Little Newly formed bone was observed around the grafted bone particles, which were dispersed above the bone bed in all groups. No membrane remnants were observed in any samples of the NCM group. In contrast, partially resorbed DCM leaflets exhibiting structural integrity were clearly identified between the gingival connective tissue and bone substitute materials in the DCM group at magnifications of 100- and 200-fold (Figure 3). Inflammatory processes were not considered to be present in either group, and so these histological results indicate that DCM exhibited sufficient biocompatibility.
Figure 3
Histological images from the DCM group at the time of re-entry surgery. (A, B) Partially resorbed collagen membrane leaflets exhibiting structural integrity and some blood vessels (BVs) were observed. Bone substitute materials (BM) were surrounded by collagen membranes and BVs. New bone (NB) formation was observed on the BM surface. (A: Masson's trichrome stains, ×100, Scale bars, 500 μm; B: Masson's trichrome stains, ×200, Scale bars, 200 μm).

DISCUSSION
The aim of this study was to determine the clinical feasibility of using DCM compared with NCM for treating human peri-implant dehiscence defects. Both types of collagen membrane demonstrated significant improvements in all clinical and radiographic parameters, with no signs or symptoms of severe complications during the postoperative experimental period.
The horizontal and vertical dehiscence defects did not differ significantly between the DCM and NCM groups at baseline. Re-entry surgery was performed after 16 weeks, at which time the clinical condition of the defects was considered to be acceptable, thereby confirming the successful occurrence of GBR. Premature exposure of membranes was found in two samples in the NCM group (14.3%) and three samples in the DCM group (21.4%). It is generally known that soft-tissue dehiscence defects and exposure of membrane lead to impaired bone healing and significant deterioration of the defect [2324]. However, notable reduction of bone regeneration and impaired wound healing was not observed in the DCM group. This is consistent with the finding of Moses et al. [25] that a cross-linked collagen membrane was advantageous for GBR procedures. The results obtained in the previous and present studies together indicate that the cross-linking method prevents biodegradation of the collagen membrane and promotes soft-tissue healing without any signs of infection during the secondary healing period [2526].
The measurements of HT1, HT2, and HT3 revealed decreases at 16 weeks in both groups compared to baseline, but there were no statistically significant intergroup differences. The bone density of HT1 was measured using CBCT to predict the quality of bone remodeling. The average bone density in both groups was within the general acceptable range (D1 to D3) for bone quality [27]. Regardless of the presence of premature membrane exposure, no significant radiographic or clinical differences were evident.
Histological analyses revealed that the NCM applied at the defect site was significantly absorbed at 4 weeks and almost completely absorbed at 16 weeks [28]. NCM reportedly shows rapid degradation and good biocompatibility, whereas physically cross-linked membrane shows slow degradation but with a similarly low cytotoxicity [2930]. However, it was difficult to verify these findings with the histological results obtained at 16 weeks in the present study. The remaining unabsorbed DCM fragment was observed histologically only in the DCM group, whereas no NCM fragments were observed in the NCM group. This histological result for the DCM group was similar to that for the NCM group and it confirmed the presence of good biocompatibility. However, because this study conducted biopsy sampling in the keratinized gingival tissue zone above the cover screw, the amount of new bone and pattern of bone resorption could not be evaluated, and only some grafted bone particles and integration into new bone were observed.
Depending on the type, structure, degree of cross-linking, and surface-treatment method, it is crucial to determine the mechanical, chemical, and physical properties of the collagen membrane [1131]. The DHT cross-linking technique increases the number of amino-acid side chains between collagen molecules and unwinds the triple-helix structure of collagen [32]. The fibroblast binding sites (α1β1 and α2β1 integrins) are subsequently modified, but it is not yet clear if these physical changes determine the major mechanical and biochemical characteristics of DCM [933]. Compared to the conventional DHT cross-linking method, which requires 3 to 5 days of dehydration, the collagen membrane used in the present study was dehydrated at 100°C under vacuum pressure (1 torr), which reduced the dehydration period to 24 hours. Like the physical cross-linking method using UV radiation, this represents a more effective and rapid cross-linking method [32].
The previous and present studies found that DCM was stiffer and more hydrophobic than DCM, which is attributable to the increased binding between the carboxyl and amino groups of the adjacent collagen molecules [3334]. Despite the constraints of the cross-linking technique, when performing GBR at the time of implant placement it was found that the membrane could be easily manipulated, without any significant differences between the two groups. While there was a statistically significant difference in the clinician’s subjective judgement of the maintenance of localized bone particles, there was no clinically meaningful difference in the VAS score between the NCM (0.3±0.7) and DCM (1.3±1.1) groups (P=0.119). Therefore, clinicians can use the DHT cross-linking method to control the biodegradation rate of the membrane, allowing the easy and effective use of DCM to achieve successful bone augmentation.
In this study, the different types of implants fixtures had the same SLA surfaces with bone level fixtures; in other words, they had very similar designs and surfaces. A recent systematic review revealed no significant difference between SLA implants types in success rate or marginal bone loss [35]; therefore, although this may pose as a limitation, its effect can be assumed to be minimal. Moreover, the change in bone graft material during the study that was necessitated by our parallel research findings also acts as a limitation. Despite the limitations, the present randomized clinical study indicates that the clinical expediency, biocompatibility, and more enhanced degradation resistance are similar for DCM and NCM. DCM can therefore be used for GBR around serious peri-implant defects.
 XML Download
XML Download