

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The The application of an implant-supported prosthesis to treat maxillary and mandibular complete edentulism is capable of having a major impact on patients’ quality of life and on their masticatory and phonetic performance following the resolution of the functional limitations caused by edentulism [1234].
However, severe atrophy of the jaws can limit the possibilities for placing dental implants. In such cases, the necessity to increase bone volume through grafting procedures could have a negative effect on the patient’s perception of the treatment, as well as on the economic cost of treatment, due to the likelihood of a longer treatment time and the increased possibility of surgical complications, among other factors [5].
Under particular clinical conditions, the use of tilted implants combined with upright implants can be applied for the rehabilitation by fixed prosthesis of completely edentulous arches, thereby restoring masticatory and aesthetic functionality while avoiding the need to perform bone grafting procedures [6, 7]. In this way, dental implants can support a full-arch prosthesis that may also compensate for the consequences of atrophy, with the goal of restoring adequate support to the lips and correcting the vertical dimension [8].
A number of studies have evaluated the clinical results of rehabilitations supported by a combination of tilted and upright implants [91011]. This kind of restoration has been reported to have a high implant survival rate, ranging from 97.2% to 100%. However, technical and biological complications can occur, although appropriate interventions are capable of significantly limiting the prevalence of implant or prosthesis failure [12, 13].
Significant debate has emerged regarding the definition of implant survival and success criteria for implants [14]. In general, we considered functional implants without evident mobility to have survived, in accordance with several studies that have used these criteria to validate both short- and long-term data [15161718]. However, the major limit of considering only this parameter is that an implant may still be in place even in the presence of peri-implantitis or severe hard and soft tissue recession that could, for example, lead to complete aesthetic failure [19, 20]. Most of the criteria for implant success are related to bone resorption. Albrektsson and colleagues [21] revised the principles initially proposed by the National Institute of Health in 1979. The most important revision was related to the bone resorption rate, which should be less than 0.2 mm after the first year of loading. Another classification of implant success was proposed at the International Congress of Oral Implantology in 2008 [22]. The authors proposed that bone resorption of less than 2 mm, as detected through periapical radiographs, and the absence of any signs or symptoms of mobility after prosthetic loading should be the criteria for success. However, no classification for implant success or failure has been generally accepted.
The aim of this retrospective investigation was to explore the success and survival rate of implants supporting a full-arch rehabilitation using an immediate loading protocol in the treatment of maxillary or mandibular edentulism. Furthermore, the occurrence of biological complications was recorded and analysed.
MATERIALS AND METHODS
This retrospective clinical trial was performed following the principles articulated in the Helsinki Declaration and further modifications [23]. The Review Board of the Oral Implantology Research Centre of the Università degli Studi di Milano in Milan, Italy approved the study protocol in 2013 (Protocol 1. 2013).
The inclusion criteria were:
- Patients treated with full-arch rehabilitations supported by a combination of two tilted and two upright implants, with the prosthesis placed following an immediate loading protocol (within 48 hours from surgery), which was chosen in order to avoid the need for bone regeneration procedures in the posterior areas of the jaws;
- Patients who had radiological documentation in the form of periapical radiographs for each implant and for each follow-up visit;
- Patients whose clinical data demonstrated at least adequate oral hygiene (a full-mouth plaque score of less than 25% and a full-mouth bleeding score of less than 25%, calculated by computing the proportion of teeth surfaces presenting plaque and bleeding, respectively [24]).
The exclusion criteria were:
- Patients who were missing radiographs (either at baseline or at follow-up appointments) or clinical data;
- Patients who failed to attend the planned follow-up visits.
Outcomes
The primary outcome was the cumulative implant success rate (CSR) evaluated for each implant according to the classifications used in this study (Table 1): the Albrektsson classification [21] and the Misch classification [22]. Each implant was classified as successful or not successful after evaluation of the clinical records and the periapical radiographs, taken using a paralleling technique and an individual X-ray holder. All measurements were performed by two expert and calibrated operators (AR, SC) independently, and in cases of disagreement, a third operator was consulted. Measurements were made using the Image-J analysis software (NIH Image-J v.1.45s; US National Institute of Health, Bethesda, MD, USA).
Table 1
Criteria for defining implant success.

| Misch et al. [22] | Albrektsson et al. [23] |
|---|---|
| 1. No pain or tenderness upon function | 1. Absence of mobility |
| 2. No mobility | 2. Absence of any evidence of peri-implant radiolucency |
| 3. Less than 2 mm of radiographic bone loss after initial surgery | 3. Vertical bone loss be less than 0.2 mm annually following the implant's first year of service |
| 4. No history of exudates | 4. Absence of pain, infections, paraesthesia, or violation of the mandibular canal |
The secondary outcomes were:
- The implant survival rate, based on a calculation of the number of functional implants;
- The occurrence of peri-implantitis. Peri-implantitis was defined as the presence of radiographic bone loss and clinical signs of marginal inflammation, such as bleeding on probing, swelling, and increased probing depth.
Statistical methods
The prevalence and incidence of unsuccessful implants and patients was computed for each 12-month time frame within the overall five-year follow-up period, as well as the implant survival rate. The life-table analysis method was used to compute cumulative success rates for both classifications and for both jaws [25]. Briefly, given ni, the number of implants in the interval; di, the number of implants not successful in an interval; and wi, the number of implants withdrawn; pi, the probability of surviving during the interval, was computed as follows: pi = 1 − (di − ni*) where ni* is computed as ni* = ni − 0.5 * wi. The cumulative success rate was then CSR = p1 * p2 * … * pk
Differences in the number of unsuccessful and successful implants depending on orientation (tilted or upright) and between the Misch and the Albrektsson classifications were computed using Fisher’s exact test. P-values <0.05 were considered to indicate statistical significance.
RESULTS
A total of 212 implants (53 full-arch rehabilitations) in 46 patients were evaluated in the first 12 months of follow-up. Eighty-eight implants supported maxillary restorations, while 124 supported mandibular restorations. Twenty-nine patients were female, and the mean age for all subjects was 61 ± 12 years at the time of the first follow-up visit.
The CSR five years after implant/prosthesis placement was 62% for maxillary implants and 82.6% for mandibular implants using the Misch classification (Table 2). When maxillary and mandibular restorations were considered together, the CSR was 97.92% after one year, 91.98% after two years, 86.62% after three years, 81.67% after four years, and 76.04% after five years, using the Misch classification. Using the Albrektsson classification, the five-year CSR was 43.4% for maxillary implants and 63.6% for mandibular implants (Table 3). When maxillary and mandibular restorations were considered together, the CSR% was 90.95% after one year, 85.44% after two years, 78.08% after three years, 67.39% after four years, and 56.34% after five years, using the Albrektsson classification. One of the cases examined in the present study is presented in Figure 1.
Table 2
Cumulative success rate for maxillary and mandibular restorations, following the classification of Misch [22].

Table 3
Cumulative success rate for maxillary and mandibular restorations, following the classification of Albrektsson [21].

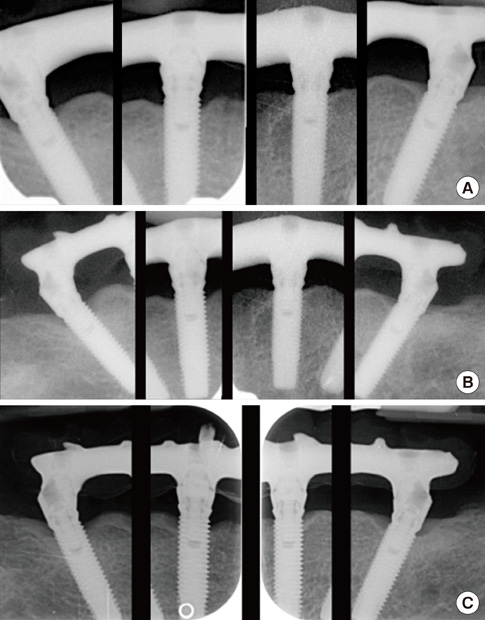
Figure 1
(A) Baseline findings of a patient. (B) Follow-up image taken three years after implant and prosthesis placement, showing no evidence of significant marginal bone resorption. (C) Follow-up examination at five years. No relevant marginal bone resorption was detected.

One implant in one patient showed signs and symptoms of peri-implantitis in the 12–24-month time frame. The cumulative implant survival rate was 100% (Table 4).
Table 4
Incidence of peri-implantitis and implant survival rate.

No statistically significant differences were found in the success rate between tilted and upright implants. However, in the first 12 months of follow-up alone, a statistically significant difference was found between the number of implants classified as successful following the Misch classification and those classified as successful following the Albrektsson classification (P=0.0034).
DISCUSSION
In the present retrospective investigation, the implant survival rate was 100%, whereas the CSR, determined using both classifications, dropped gradually over time, meaning that significant physiological changes took place even in the absence of a significant prevalence of peri-implant infectious disease, such as peri-implantitis.
The vast majority of implants judged as unsuccessful in each time frame showed a marginal bone resorption higher than judged acceptable by a given classification. Nevertheless, marginal bone resorption was caused by peri-implantitis in only one implant in one subject. Therefore, in the other subjects, marginal bone resorption was most likely due to the physiological rearrangement of marginal bone over time.
A systematic literature review by Patzelt et al. [11] reported data about the same treatment strategy that was evaluated in this study. A total of 13 studies were included, and the reported implant survival rate at 12 months ranged from 97.2% for maxillary restorations [26] to 100%, which has been reported in multiple studies [15, 18, 27-30]. With regard to marginal bone loss, previous studies have generally reported no differences between upright and tilted implants, corresponding to the results of the present study. The reported pooled marginal bone loss was 0.9 ± 0.5 mm at 12 months, 0.9 ± 0.4 mm at 24 months, and 1.3 ± 0.4 mm at 36 months. These mean values of marginal bone resorption exceed the values proposed by Albrektsson and colleagues [21], which is why a lower number of successful implants was found using their classification than when the Misch classification was used [22].
Another systematic literature review focused on the differences in bone resorption between upright and tilted implants [9], reporting no statistically significant differences in a meta-analysis, which supports the results of our investigation. Moreover, the authors reported that, at 12 months of follow-up, the mean resorption rate for axial fixtures ranged from 0.43 ± 0.45 mm [31] to 1.13 ± 0.71 mm [32], while for tilted fixtures, it ranged from 0.34 ± 0.76 mm [33] to 1.14 ± 1.14 mm [32]. These results are comparable to those reported in other reviews.
Our study found no correlation between the CSR and the implant survival rate over time. An implant can be considered to have survived if it is still present in the mouth and supports a prosthesis, which is independent from the issue of potential hard and soft tissue resorption [34]. Therefore, the survival rate overestimates the true status of an implant and can be considered as of low significance in clinical practice.
In the present study, the occurrence of technical and biological complications was not analysed quantitatively. Even though most technical and biological complications could be successfully treated without influencing the survival of the prosthesis, their occurrence may have been high, as reported in a previous literature review [13], and they could have had an impact on patients’ perceptions of their treatment. In a previous study, prosthetic veneer fractures were reported to occur in 33.3% of patients after five years, while the occurrence of more than 2 mm of bone loss was reported in 20.1% of the 1392 implants that were evaluated. Those results are comparable to the findings of our study using the Misch classification, confirming a tendency for marginal bone resorption over time.
Some limitations in the present study should be considered. First, the retrospective design of the protocol may have significantly limited the external validity of the results. Second, we chose to use two of the most commonly used classifications for implant success, but many others have been proposed [14], and no clear agreement has been reached regarding this issue. Finally, the exclusion of some data due to incompleteness could have confounded our results.
In conclusion, considering the limitations of this study, we can conclude that implant success criteria did not reflect the actual condition of the implant-supported restorations, as marginal bone resorption was not associated with peri-implant infectious diseases. Implant loss was not related to the occurrence of a bone resorption rate higher than would be considered successful according to two commonly used sets of criteria for implant success.
 XML Download
XML Download