

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
There has been an increasing need for dentists to gather subjective and objective information about the masticatory function of patients before and after dental treatment. Masticatory ability, which is generally assessed by subjective evaluation, is defined through questionnaires designed to assess masticatory function with respect to diverse foods. A previous study demonstrated that the food intake ability (FIA) score is a useful indicator reflecting the various physical properties of foods [1]. There have also been diverse approaches to the objective assessment of masticatory performance. Among these, Sato et al. [2] proposed the use of artificial food composed of two-color utility wax cubes and formulated a mixing ability index (MAI), scores of which are determined by the degree of color-mixing and the shape of the wax after chewing. Several previous studies have reported that the FIA and MAI scores can successfully evaluate masticatory function in patients with temporomandibular disorders or botulinum toxin injections and in orthodontic patients [345].
In general, the success rate of dental implants is assessed according to clinical parameters such as stability and radiographic bone loss [6]. However, patients often find dental terminology difficult to understand. From the patient’s point of view, the success of the prosthodontic treatment depends on their ability to chew well. Therefore, an evaluation of the changes in masticatory function is more appropriate than typical histological approaches.
Some previous studies have used alveolar bone loss or implant movement to evaluate implant success over a relatively long follow-up period, e.g., several years after the implant restoration [789]. However, most patients use their prosthodontic implants to chew food only a few days after undergoing implant surgery. Recently, immediate placement and immediate loading have become popular in implant dentistry, as patient demands for timesaving procedures and immediate satisfaction have increased [10]. Hence, it is important to evaluate the changes in masticatory function over a short period of time.
Unfortunately, there has been a lack of research on the subject, and claims that mastication can be improved within a short period after implant restoration have not been thoroughly investigated. In addition, masticatory function may be expected to differ according to the status or condition of the patients’ remaining teeth, even if they only have one or two missing teeth. It can be assumed that implant restoration causes a substantial change in patients with relatively low masticatory ability.
Therefore, the first aim of the present study was to compare masticatory function among patients with two missing molars both before and two weeks after implant restoration, using both objective and subjective evaluation methods. The second aim was to compare the differences in masticatory function according to the initial edentulous masticatory status of the patient.
MATERIALS AND METHODS
Subjects and experimental procedure
A total of 54 adult patients scheduled to receive dental implant restoration between September 2012 and June 2013 at a local dental clinic in Seoul, Republic of Korea, were invited to participate in the study. The study was approved by the Institutional Review Board of the Yonsei Dental Hospital (IRB 2-2012-0029). All patients received prior verbal and written information and signed a consent form voluntarily.
The inclusion criteria targeted patients (i) aged between 20 and 70 years in the initial records and, (ii) with missing first and second molars. Patients with fixed restorative materials (e.g., crowns or bridges) were considered to have normal teeth. The following patients were excluded: those who (i) had abnormal mastication due to any oral pain, temporomandibular disorder, or severe malocclusion; (ii) had lost teeth on crowns due to severe caries; (iii) were pregnant; or (iv) had a severe systemic disease such as diabetes or cardiovascular disease.
An implant fixture was placed at the site of the missing teeth and the state of the implant-bone integration examined in every subject prior to participation in the study. The date of the implant restoration and the edentulous period were different among subjects. One dentist examined each patient’s mouth and created examination records. Each subject filled out a self-assessed chewing ability questionnaire to evaluate FIA, as in Kim et al. [1]. After completion of the questionnaire, subjects chewed the two-colored paraffin wax used to measure the chewing ability [2]. All other implant materials, including abutments and prostheses, were then installed onto the implant fixture in the patients’ mouths. A recall examination was performed two weeks later.
Assessment of food intake ability
To compare subjective mastication before and after the implant restoration, a self-reported questionnaire about 30 food items divided into three groups (hard, medium, and soft) was used [1]. Subjects answered each question in the FIA questionnaire according to a Likert scale, as follows: 0 points – “have never eaten”, 20 points – “cannot chew at all”, 40 points – “difficult to chew”, 60 points – “cannot say either way”, 80 points – “can chew some”, and 100 points – “can chew well”. The total FIA score was calculated from the average score for the 30 foods.
Mixing ability index evaluation
To evaluate the objective masticatory performance, a mixing ability test was performed using wax cubes representing artificial foods, as previously suggested by Sato et al. [2]. Red and green 2×2×12 mm3-sized utility wax rods (Daedong Industrial Co., Ltd, Daegu, Korea) were placed side by side to make a sheet of 2×12×12 mm3 in size. Six identical sheets were then stacked to generate a lattice cube of 12×12×12 mm3 in size. The wax cubes were stored at 4°C to preserve their properties until use. Subjects were required to chew one wax cube over 10 strokes in a habitual manner. This procedure was repeated twice. The chewed waxes were carefully removed from the mouth, washed with water, and dried at room temperature.
The total number of wax samples was 108. Digital images of the dried waxes were captured with a digital single-lens reflex (DSLR) camera (D80, Nikon Co., Tokyo, Japan) using standardized distance and light conditions. A total of 216 digital images were obtained by taking photographs of the front and back surfaces of the wax samples. All images were saved as JPEG files and an image analyzer (Image-Pro plus® v6.0, Media Cybernetics Inc., Bethesda, MD, USA) was used to determine the color and shape of the wax on each surface. On each image, an examiner selected the unmixed red and green colors using the eyedropper tool built into the analyzer. Subsequently, the parameters of the captured images for each wax cube were analyzed, including the total projection area, the projection areas of less than 50 µm in thickness, the maximum length, and the maximum breadth. The MAI score was calculated using the above parameters, as described in a previous study [11], and then converted into a percentage scale from 0 to 100.
To compare the objective masticatory efficiency, MAI groups were subdivided into good and poor MAI groups based on a cutoff MAI score of 50 points before restoration.
Statistical analysis
A frequency analysis was performed to confirm the distribution of each score. A paired t-test was used to compare between before and after the implant restoration of the FIA or MAI. A one-way analysis of variance (ANOVA) was applied to identify the significant differences in each score according to different food properties. A two-sample t-test was used to identify differences in the mean value of each score in each MAI group before and after the implant restoration. All statistical analyses were carried out using PASW statistics, Version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
The average age of the 54 patients enrolled in the study was 51.6±12.3 years old, and 32 patients (59.3%) were female. The two indicators of masticatory function (the FIA and MAI) showed significant increases after dental implant restoration, presumably as a result of recovery at the site of the missing molars (Table 1, P<0.0001). According to data analyzed from 54 patients, there was an increase of 9.0% in the FIA, compared with the edentulous state, when examined two weeks after the implant restoration. The MAI showed a 14.3% increase.
Table 1
Changes in masticatory function before and after dental implant restoration.

| Before | After | Difference | P-value | |
|---|---|---|---|---|
| FIA | 82.73±8.63 | 90.16±7.41 | 7.43±7.68 | <0.0001 |
| MAI | 54.72±14.12 | 62.54±13.30 | 7.81±11.00 | <0.0001 |
The average FIA increased for all three food group following implant restoration, with the hard food group demonstrating the largest mean increase (10.8%, P<0.0001), followed by the medium food group (10.0%, P<0.0001), and the soft food group (3.7%, P=0.015) (Table 2).
Table 2
Changes in FIA before and after dental implant restoration according to food property.

| Food group | Before | After | Difference | P-value |
|---|---|---|---|---|
| Hard | 79.74±7.32a) | 88.35±4.29a) | 0.53±0.10a) | <0.0001 |
| Medium | 80.25±7.32b) | 88.27±3.81a) | 0.28±0.17b) | <0.0001 |
| Soft | 93.01±6.41c) | 96.44±3.61b) | 0.12±0.79b) | 0.015 |
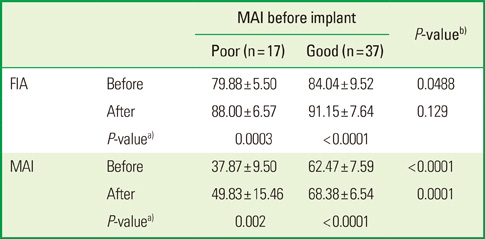
In comparison with the good mastication group, which presented MAI scores over 50 before restoration, the increases in subjective and objective masticatory efficiency in the poor mastication group were higher. After the implant restoration, the average increase in the MAI score as compared with the edentulous state was largest in the poor MAI group at 31.6%, and the average FIA score was increased by 10.2%. In contrast, the average increase in the MAI score in the good MAI group was only 9.5%, and the average increase in the FIA score was 8.5%. In other words, the improvement ratio for masticatory function after implant restoration showed a greater change when measured with the MAI (about 2.0-fold) than in with FIA (1.2-fold) (Table 3).
Table 3
Masticatory function before and after dental implant restoration according to pre-implant MAI score.

DISCUSSION
The reduction of masticatory function from tooth loss can cause significant problems, including difficulties with food mixing and swallowing [12]. For patients with a missing tooth in the molar area, dental implants are considered as the primary option. However, the improvement of masticatory function in patients with implant restoration has not previously been measured with both subjective and objective masticatory evaluations.
The current study identified changes in masticatory function before and after implant restoration in the molar area. A self-evaluation FIA questionnaire was used to measure the inconvenience associated with chewing food and to examine the change in masticatory function after implant restoration. The other objective assessment tool was the MAI test, which uses two-color wax cubes to obtain quantitative analysis parameters of the various changes in masticatory function following implant restoration [1].
We evaluated changes in masticatory function in order to understand the short-term improvement gained from an implant restoration. Two weeks is a relatively short period of time to evaluate masticatory function, particularly when compared with previous studies that evaluated masticatory function between two weeks and five years after restoration with removable dental prostheses or partial implant fixed dental prostheses [131415]. However, we specifically aimed to assess immediate to short-term improvement in masticatory function gained from an implant prosthesis. Dental implant restoration has been used for several decades to address patients' needs for immediate functional and aesthetic rehabilitation. It is important for patients to experience immediate success; however most prior studies have only evaluated the survival rate of the implant restoration after long periods of time [1617]. Awad et al. [18] and Reisine et al. [19] reported that the oral health-related quality of life of patients with implant prostheses increased rapidly. In keeping with these findings, the present study gives evidence for short-term improvement of masticatory function after implant restoration.
The mean FIA scores after the implant restoration were increased in all groups (Table 2), and particularly in the hard food group. The difference in the FIA score before and after restoration was lowest in the soft food group. Lucas and Luke [20] reported that the mastication of hard or tough foods could be improved more easily than that of soft foods. Correspondingly, the participants in the current study clearly identified a subjective change in the mastication of hard foods but could not easily evaluate the convenience of mastication of soft or medium hardness foods (Table 2).
In a previous study, the MAI score was reported as a normal distribution in a population of 147 Korean adults [11]. In the present study, the MAI score was mathematically converted into a 0-to-100 scale, as the original MAI value, which calculated from discriminant function, was not easy to interpret. A mean MAI score of 54.7 was measured prior to the implant restoration. This is similar to the previous study, which evaluated masticatory function related to molar tooth loss using a method identical to the one employed in this study and found an MAI score of 53.4 in patients with one or two missing post-canine teeth. Moreover, the MAI score after implant restoration in the present study was 62.5, which was similar to the MAI score of 61.9 for those who had lost no teeth in the previous study [11]. Although the duration of time before and after the implant restoration was small, it was nevertheless sufficient for recovery of the decreased mastication caused by one or two missing teeth. Similarly, Kim et al. [21] also showed an increase in masticatory function after a second single molar implant treatment.
The improvement rate was dependent on the masticatory state before restoration (Table 3). When subjects were divided into good and poor masticatory function groups, based on an MAI score of 50.0 before restoration, the improvement rate was higher in the poor MAI group than in the good MAI group. In addition, the significant difference in MAI or FIA scores between the poor and good groups that existed before restoration decreased after the implant restoration. The MAI showed around a two-fold higher improvement than the FIA. Taken together, these results indicate that patients with low masticatory ability have a higher rate of recovery of masticatory function after implant restoration.
Previous studies have reported a moderate correlation (r=0.40) between objective masticatory performance and subjective masticatory ability [111]. In the present study, a moderate correlation between the FIA and MAI was observed both before (r=0.37) and after (r=0.29) the implant restoration. Therefore, both subjective and objective methods of masticatory evaluation should be considered as necessary complementary.
There were several limitations to the present study. Oral conditions such as caries, hypersensitivity, crack, and periodontitis, which could affect implant placement, were not considered as exclusion criteria. In addition, we did not consider other restorative materials in the remaining dentition, although these could have affected masticatory function [1418]. Likewise, the bite force is also strongly related to mastication and oral conditions. Moreover, although previous studies have reported that the area of tooth loss is more important than the number of residual teeth, this was not evaluated in this study as the masticatory procedure is dynamic and includes tongue, cheek, and tooth movements [2223]. Therefore, complex oral conditions need to be considered in future studies.
In conclusion, this study confirmed that masticatory function, as evaluated with subjective FIA and objective MAI methods, could increase two weeks after implant restoration. The enhancement of masticatory function was particularly high in patients with poor mastication before the implant restoration.
 XML Download
XML Download