

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The esthetic rehabilitation of missing teeth in the maxillary anterior region is often plagued with problems, such as uneven tooth recovery and issues related to the gingiva in adjacent teeth [12]. Alveolar ridge resorption following a tooth extraction is inevitable, and continues throughout the patient's lifetime [34]. Eventually, papilla loss and atrophy of the residual ridge compromise esthetic outcomes. These undesirable consequences present challenges when restoring the maxillary anterior esthetic region with conventional prostheses. Pink porcelain restorations and surgical socket preservation techniques have been used to compensate for compromised tissue [2]. However, neither technique has solved the problem of compromised esthetic outcomes by ensuring predictable results [2567].
The root submergence technique preserves the periodontium surrounding a root without requiring an extraction [89101112131415]. A submerged root maintains the periodontal attachment complex, preventing the resorption of the alveolar bone on the buccal and lingual walls, as well as on the interproximal area [913]. As a result, this technique maintains the dimension of the alveolar ridge and the surrounding tissue [912131415]. Root submergence was first introduced to prevent residual alveolar ridge resorption in order to increase the retention and resistance of a complete denture [8]. Clinical and histological studies found that non-infected vital or endodontically treated roots reduced at the level of the bone crest or below the crest and completely submerged within the alveolus were able to effectively preserve the residual ridge [91011]. Recently, this concept has also been applied to rehabilitation with fixed dental prostheses [12131415]. Under the pontic site, a root was retained at the crestal bone level to preserve ridge form and no exposure of the root was expected, due to the absence of direct pressure over it [12]. The root submergence technique has also been applied in implant-supported prostheses in the maxillary anterior region [131415]. Although successful esthetic outcomes without papilla loss or collapse of the arch have been reported, the long-term results of the root submergence technique have not been published.
This clinical report describes a root submergence technique employed to develop the pontic site of a fixed dental prosthesis in the maxillary anterior aesthetic zone.
CASE DESCRIPTION
Case 1
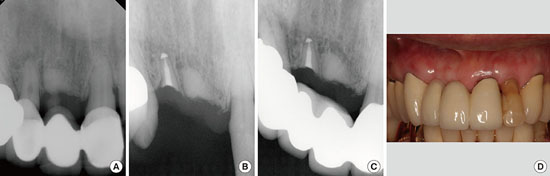
A 63-year-old male patient presented to the clinic with the complaint of movement in a maxillary anterior prosthesis that had been placed five years ago. Clinical and radiographic examinations revealed that his maxillary right lateral incisor, used as the abutment tooth for a three-unit fixed dental prosthesis, had a secondary caries with inadequate structural support, causing bucco-lingual movement of the prosthesis. A noteworthy finding in this prosthesis was a maxillary right central incisor root remnant, which had been covered by soft tissue and remained for five years underneath the pontic site (Fig. 1A). The radiographic and clinical evaluation showed no inflammation, dehiscence, external root resorption, or any known pathologies, and the arch form was maintained without any sign of ridge deformation. It was evident that a submerged root of the maxillary right central incisor had prevented bone resorption, especially in the interproximal area. Due to the severe secondary caries, the prognosis for the maxillary right lateral incisor was poor: it was thus submerged as a root remnant at the pontic site. The tooth was endodontically treated due to the periapical lesion, then decoronated at a crestal bone level similar to that of the maxillary right central incisor. No surgical intervention was performed, and an interim fixed dental prosthesis supported by the maxillary right canine and maxillary left central incisor was fabricated, relieving pressure on the soft tissue under the pontic sites. After a three-month healing period, the root was completely covered by soft tissue, and the periapical lesion was disappeared (Fig. 1B). No noticeable changes were observed in the alveolar ridge of the pontic site either vertically or horizontally. Upon completion of the healing process, a metal ceramic fixed dental prosthesis was fabricated and cemented with a resin-modified glass-ionomer cement. Since the submerged roots preserved the bone and soft tissue, the gingival contour of the pontic site was in harmony with the gingival margins of the adjacent abutment teeth. At a two-year follow-up visit, the bone level at the submerged root site was stable, and the gingival contour under the pontic site was maintained (Fig. 1C, D). The patient was satisfied with the outcome of the prosthetic rehabilitation.
Case 2
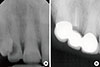
An 83-year-old male patient presented with a gross caries on the disto-cervical surface of the maxillary right lateral incisor with food impaction and discoloration. Clinical and radiographic evaluation indicated that the tooth was non-vital, and that the cavity extended to the crestal bone level (Fig. 2A). Among several treatment options, ranging from a post-and-core crown to implant placement following a tooth extraction, the patient decided to submerge the root of the lateral incisor and undergo restoration with a three-unit fixed dental prosthesis. The prosthesis was intended to have the additional benefit of addressing severe attrition in the adjacent maxillary right central incisor and canine. Single-visit endodontic treatment was performed on the maxillary right lateral incisor, with decoronation at the level of the alveolar crest. No soft tissue augmentation was performed on the decoronated area, and the root was completely covered by gingival tissue five months after the decoronation procedure. A three-unit metal ceramic restoration was fabricated and cemented with a resin-modified glass-ionomer cement. At a three-month follow-up visit, the architecture of the hard and soft tissue was found to have been preserved at the pontic site, and no pathology was noted (Fig. 2B).
Case 3
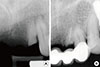
A 51-year-old male patient presented to the clinic with a fractured maxillary left lateral incisor tooth and severe toothache. The patient had previously experienced severe periodontitis and had lost the maxillary central incisors, resulting in a compromised residual ridge. The radiographic and clinical examination indicated a poor prognosis for the maxillary left lateral incisor, due to a compromised crown-to-root ratio and exposed pulpal tissue (Fig. 3A). The maxillary left lateral incisor had a peg lateralis shape and was not a suitable retainer tooth for the planned fixed dental prosthesis. Rather than using the maxillary lateral incisor as an abutment tooth, the fixed dental prosthesis was extended to the maxillary left canine, with the maxillary left lateral incisor submerged in order to preserve the already compromised ridge. After a single-visit root canal treatment and root decoronation to the crestal bone level, the root was completely covered by soft tissue within six months. Upon completion of the healing process, no signs of inflammation or dehiscence were noted, although minimal interproximal bone loss had taken place. A five-unit metal ceramic fixed dental prosthesis was fabricated, and the patient underwent follow-up 24 months later (Fig. 3B).
DISCUSSION
Atrophy of the residual ridge following extraction of a hopeless tooth compromises the final esthetic outcomes, especially in the maxillary anterior region. As long as the hopeless tooth has no periapical pathology, its root remnant can be submerged to preserve the surrounding periodontal tissue [9]. The root submergence technique was first developed to preserve the periodontal attachment complex, in order to increase the retention and stability of removable prostheses. Several studies have reported the successful preservation of periodontal tissue with vital or endodontically treated roots covered by bone or soft tissue [9101116]. Submerged roots between dental implants have also been found to preserve the gingival architecture and prevent interproximal bone resorption [131415]. Otherwise, the proximity of the implant fixtures in case with multiple missing teeth could cause accelerated bone resorption. Retaining the gingival contour is one of the most significant factors in the esthetic rehabilitation of the maxillary anterior region; ridge atrophy is therefore a major culprit in the creation of esthetically unfavorable outcomes [2].
This clinical report describes the application of a root submergence technique to develop the pontic site of a fixed dental prosthesis. It was found that a submerged root underneath an old three-unit fixed dental prosthesis preserved the surrounding periodontium for five years without any periapical pathology (Fig. 1A). These findings indicate that the root submergence technique could serve as an effective alternative treatment to socket preservation of a pontic site, with or without tissue augmentation procedures. All submerged roots that were decoronated were completely covered by soft tissue after healing and showed no changes in two-year follow-up evaluations.
Other studies have reported several complications such as periapical lesions, external root resorption, ankylosis, and root caries if a root is not completely covered, or if soft tissue perforation occurs under functional removable prostheses [17]. Such complications could result in extraction of the submerged roots and require multiple procedures to salvage the area. Therefore, precise clinical and radiographic examinations before and after the root submergence procedure are critical to prevent such complications [1418].
With caution, the root submergence technique could serve as a promising method of maintaining the dimensions of the alveolar ridge at the pontic site of a fixed dental prosthesis in the maxillary anterior esthetic zone. More longitudinal follow-up studies are needed to evaluate the long-term outcomes of this technique.

 XML Download
XML Download