

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recombinant human bone morphogenetic protein-2 (rhBMP-2) is a highly effective tool in bone engineering in the field of dentistry [1234567]. The United States Food and Drug Administration (FDA) has approved the use of rhBMP-2 for dental use in extraction sockets and the maxillary sinus. Clinical trials for those indications have demonstrated the safety and effectiveness of rhBMP-2 in these applications [89]. In addition, the off-label use of rhBMP-2 was reportedly effective for overcoming severely defective situations [67].
There have been false and exaggerated reports regarding the safety of rhBMP-2 in spinal fusion surgery [10]. Compared to industry-sponsored publications, much higher complications were found for the same study population in FDA documents. Although clinical studies from the dental field have found no noteworthy complications [811], adverse effects associated with high doses of rhBMP-2, such as ineffective new bone formation, implant dislocation, and void formation, have been found in preclinical studies [1213]. Thus, the minimal dosages of rhBMP-2 needed for bone regeneration has been investigated [1414151617].
The optimal delivery of rhBMP-2 requires the selection of an appropriate carrier. The absorbable collagen sponge (ACS) was the first approved carrier, and its clinical efficacy has been demonstrated in human trials [9]. However, its structural durability was questioned in some situations [1819]. Moreover, it was shown that the initial burst-release pattern obtained with ACS may lead to potential adverse effects [20] and may not be beneficial in sustaining bone-inducing activity [4].
Collagenated biphasic calcium phosphate (CBCP) has recently received attention in the dental field [421]. As a bone substitute, CBCP shares the same basic characteristics of biphasic calcium phosphate (BCP), and exhibits comparable bone-regenerative potential [2223]. As a carrier for rhBMP-2, the effectiveness of both BCP and CBCP has been demonstrated independently in several animal studies [342124]. Both carriers were found to enhance new bone formation without hampering volume stability.
The addition of collagen to BCP may confer added benefits in bone regeneration. Collagen absorbs blood easily, and may create a favorable matrix for bone formation together with the network of BCP particles [25]. Previous studies have demonstrated that adding a collagen coating to a ceramic material enhances the proliferation rate, survival, and infiltration of osteoblasts [2627]. In addition, ACS and BCP have different patterns of rhBMP-2 release, with BCP known to retain rhBMP-2 longer than ACS [2829]; thus, the combination of both materials may result in the sustained release of rhBMP-2 [4].
The proportions of slowly resorbing hydroxyapatite (HA) and rapidly resorbing beta-tricalcium phosphate (β-TCP) in BCP are known to affect regenerative outcomes, such as new bone formation, space maintenance, and material resorption [30]. The higher proportion of β-TCP in BCP is known to result in a greater amount of new bone formation, but it may impede volume stability due to the highly resorptive characteristics of β-TCP [31]. The dependency of those behaviors on the HA:β-TCP ratio has also been simulated in CBCP [32]. It has been demonstrated that BCP with a higher ratio of β-TCP was more effective compared with a lower ratio of β-TCP when it was loaded with rhBMP-2 [1]. It is thus suspected that the strategy of loading rhBMP-2 onto CBCP containing a high ratio of β-TCP could be a way of enhancing the activity of rhBMP-2.
The objective of this study was to comparatively assess the bone regenerative capacity of three carriers loaded with a low dose of rhBMP-2: ACS, BCP and CBCP, each containing a high ratio of β-TCP.
MATERIALS AND METHODS
Characterization of CBCP
The CBCP used in this study (Osteon II collagen, Genoss, Suwon, Korea) was composed of 94-96% BCP and 4-6% collagen (by volume). The BCP in the CBCP comprised 30% HA and 70% β-TCP, and the collagen was incorporated with BCP via a coating method. The CBCP was provided in cylindrical form, with dimensions of 8 mm × 2 mm (diameter × height).
For phase analysis of the CBCP, X-ray diffraction (XRD; RigakuUitima III, Tokyo, Japan) with monochromatic Cu-Kα radiation at 40 kV and 200 mA was used; the XRD spectra were scanned at 2θ values in the range of 20°-60°. The microstructures of CBCP and BCP were observed using scanning electron microscopy (SEM; Tescan Vega II LSH, Warrendale, PA, USA).
Experimental animals
Ten male New Zealand white rabbits (14-16 weeks old, mean body weight 3.0-3.5 kg) were used for this study. The determination of the number of experimental animal followed our previous studies for evaluating bone regeneration in rabbit calvarial defects [3133]. All procedures for animal selection, management, preparation, study design, surgical protocol, and postoperative care were approved by the Institutional Animal Care and Use Committee of Yonsei Medical Center (approval no. 2011-0031).
Study design
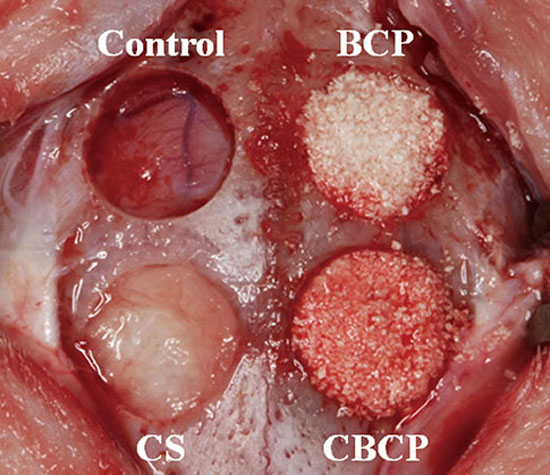
Four circular 8-mm-diameter defects were made in the calvarium of each rabbit and each of the four defects in each animal was assigned to one of the following four groups: (1) the defect was filled with blood coagulum (control), (2) the defect was filled with ACS soaked with rhBMP-2 (CS group), (3) the defect was filled with rhBMP-2-loaded BCP (BCP group), (4) the defect was filled with rhBMP-2-loaded CBCP (CBCP group). The ACS was manufactured in an 8 mm × 2 mm (diameter × height) cylindrical shape (type I bovine collagen, Genoss, Suwon, Korea).
The rhBMP-2 (Genoss, Suwon, Korea) was loaded onto each material (i.e., ACS, BCP, and CBCP) at a concentration of 0.05 mg/mL in a volume of 0.1 mL (0.005 mg per defect), and with a binding time of 10 minutes. An independent person performed the random assignment of the defects to the experimental groups in the first experimental animal; in each subsequent animal the experimental grouping was assigned by rotating them in a clockwise manner.
Surgical procedures
The rabbits received an intramuscular injection of a mixture of ketamine hydrochloride (Ketalar, Yuhan, Seoul, Korea) and xylazine (Rompun, Bayer Korea, Seoul, Korea). The surgical site was shaved and disinfected using povidone iodine, and after local anesthesia with 2% lidocaine HCl (Huons, Seoul, Korea), an incision was made along the midsagittal line from the frontal area to the occipital area. A full-thickness flap was elevated using a periosteal elevator, and four circular defects with a diameter of 8 mm were created on the calvarium using a trephine bur under copious saline irrigation (Dentium, Seoul, Korea). Each defect was grafted with the assigned experimental material (Fig. 1). The flaps were then repositioned and sutured using synthetic monofilament suture material (4-0 Monosyn, B. Braun, Melsungen, Germany). The animals were sacrificed either 2 weeks (n = 5) or 8 weeks (n = 5) postoperatively.
Specimen preparation
En-bloc sections including the defects and surrounding tissues were harvested, rinsed with sterilized saline, and fixed in 10% buffered formalin for 7 days. They were then decalcified in 5% formic acid for 14 days, gradually dehydrated in a series of ethanol solutions, and then embedded in paraffin. Serial sectioning was performed at a thickness of 5 µm, and the central-most section was selected, stained with hematoxylin and eosin, and analyzed.
Histomorphometric analysis
The specimens were examined using a light microscope (Leica DM LB, Leica Microsystems, Wetzlar, Germany), and histologic images were captured (CellSens Standard 1.11, Olympus, Center Valley, PA, USA) and saved. Histomorphometric analysis was performed with an image-processing system (Photoshop CS5, Adobe Systems, San Jose, CA, USA) by a single examiner (I.H.J.). The area of total augmentation (TA; mm2), the defect closure rate (DC; %), the area of new bone (NB; mm2), and the area of residual material (RM; mm2) were measured.
Statistical analysis
Statistical analysis was performed using SPSS software (Version 20.0, IBM Corporation, Armonk, NY, USA). The histomorphometric records of each group are presented as mean±standard deviation (SD) values. The small number of experimental animals required the use of nonparametric statistical analyses. To test the significance of differences among groups for TA, DC, and NB at 2 and 8 weeks, the Kruskal-Wallis test was used at a significance level of 0.05 and then, the Wilcoxon rank sum tests with Bonferroni correction were used for post hoc pairwise comparisons at an adjusted significance level of 0.00833 (0.05/6). The Wilcoxon rank sum tests were used for the comparison of RM between the BCP and CBCP groups at 2 and 8 weeks, and for the comparison of all parameters between the 2 and 8 weeks with a level of 0.05 considered statistically significant.
RESULTS
The phase analysis of the CBCP block is shown in Fig. 2; the 2θ values of the highest two intensity peaks were 31.8° and 31.0°. When they were compared with Joint Committee on Powder Diffraction Standards card Nos. 09-0432 (HA) and 9-0169 (β-TCP), the XRD spectrum of the collagenated BCP corresponded with the composite phases of HA and β-TCP. As shown in gross view and microscopy, CBCP was able to hold easily in both dry and wet conditions and revealed a web-like structure of collagen fibrils on the BCP particles (Fig. 3).
All of the experimental animals exhibited uneventful healing, and no inflammatory changes or allergic reactions were observed. However, the specimens from one animal assigned to the group that had 8 weeks of healing were not included in the microscopic analysis due to a technical error in the histologic processing. Thus, five and four samples were analyzed for the 2 and 8 weeks groups, respectively.
At 2 weeks, the defects in the control group were almost completely filled with soft tissues, and were depressed and flattened in shape. Minimal bone ingrowth was observed and only at the defect margins. The gross morphology of the CS group was similar to that of the control group. Bone formation started mainly at the periphery of the defects, and residual collagen was observed within them. A larger number of blood vessels was observed in the CS group than in the control group. In the BCP and CBCP groups the thickness of the original calvarial bone was mostly maintained with new bone, residual particles, and fibrovascular tissues. Bone formation was more prominent in the BCP and CBCP groups than in the CS and control groups. Generally, bone formation was more prominent in the intergranular space in the CBCP group compared to the BCP group. The CBCP group exhibited more active bone formation above the dura mater than the BCP group, and this pattern was particularly distinct in the center of the defects. The number and size of blood vessels appeared to be greater in the CBCP group than in the BCP group (Fig. 4).
At 8 weeks, the control group and CS group still exhibited a depressed morphology. Bone ingrowth from the periphery of the defects had increased, and several bony islands could be observed. There was a larger number of bony islands in the CS group than in the control group. No remnants of collagen could be seen in the CS group. In the BCP and CBCP groups, the augmented space was well-maintained, and much of the space formerly filled with residual material and fibrovascular tissues at 2 weeks was replaced by new bone at 8 weeks. New bone formation was observed around the remnant material under the skin flaps in the BCP and CBCP groups. Most of the surface of residual particles was in contact with new bone. Several osteoblasts were observed near the remnant material and the front of new bone. Many osteocytes and reversal lines were observed, along with some empty lacunae (Fig. 5).
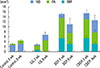
The histomorphometric results are given in Table 1 and Fig. 6. TA and NB were significantly greater in the BCP and CBCP groups compared to the control and CS groups at 2 weeks (P = 0.008 for all), but did not significantly differ among the four groups at 8 weeks. DC was significantly greater in the BCP and CBCP group compared to the control group, and was not statistically significant among the CS, the BCP, or the CBCP group at 2 weeks. At 8 weeks, a statistically significant difference in DC was not noted among the four groups. NB and DC increased significantly between 2 and 8 weeks in the control group (P = 0.014 for both) but not in the CS, BCP, or CBCP group. RM did not differ significantly between the BCP and CBCP groups at either healing time point, and decreased significantly between 2 and 8 weeks (P = 0.014 for both).
DISCUSSION
Despite a great deal of research effort, the ideal treatment modality using rhBMP-2 for bony defects has yet to be established. When using a particular dose of rhBMP-2 the various carrier systems can be similarly effective, but the efficacy may vary widely when a lower dose of rhBMP-2 is used. Thus, determination of the optimal combination of carrier and rhBMP-2 is essential. In the present study it was found that BCP and CBCP loaded with a low dose of rhBMP-2 had greater bone-forming capacity than ACS in rabbit calvarial defects, and particularly at 2 weeks post-procedure.
Our previous studies on the optimal dose of rhBMP-2 involved the testing of several doses (ranging from 0.015 mg to 0.15 mg) in rabbit models [412161718]. In the rabbit sinus, a dose of 0.15 mg loaded on BCP led to inhomogeneous bone formation (confined to the area adjoining the sinus membrane) [12], and a dose of 0.015 mg resulted in only an insignificant increase in new bone [17]. In the rabbit calvaria, the lower dose of 0.01 mg loaded on BCP significantly enhanced bone formation [16]. In the present study, the dose of 0.005 mg (the lowest dose in the studies by our group) was loaded on ACS, BCP and CBCP. New bone was significantly greater in the BCP and CBCP groups than in the control and ACS groups at 2 week, but insignificantly greater at 8 weeks. This indicates that the optimal dose of rhBMP-2 may vary depending on anatomical sites and carrier materials.
Regeneration with a high purity of target tissue requires a completely resorbing scaffold, such as ACS, but tension or pressure at the recipient site may predetermine the limit or jeopardize the immature regenerated tissue in specific situations [34]. Thus, the mechanical stability of the scaffold may also be a prerequisite, depending on the characteristics of the recipient site. The BCP and the CBCP groups in the present study exhibited enhanced space-maintaining stability compared to the CS group, which might be one of the contributing factors for greater bone regeneration. Consistent with the present study, Lu et al. demonstrated that the combination of collagen, β-TCP, and HA loaded with rhBMP-2 resulted in significantly increased new bone in the supra-alveolar peri-implant defect model compared to the ACS carrier [19].
Compared to conventional BCP, CBCP may provide a more favorable environment for bone induction. Although new bone formation in the CBCP group was not significantly enhanced at 8 weeks in the present study, an altered bone-induction pattern could be detected in the histologic sections, especially at 2 weeks. Newly formed bone in the CBCP group was found more frequently in the intergranular spaces and in the center of the defect than it was in the BCP group, which indicates that the web-like collagen network in CBCP may have enhanced the proliferation and infiltration of osteoblasts [2627] and vascular endothelial cells around [3536] and lastly strengthened the effect of rhBMP-2. This finding was also demonstrated in the canine mandibular defect model [21], whereby CBCPs with different ratios of HA and β-TCP loaded with rhBMP-2 resulted in enhanced bone formation compared to noncollagenated BCPs loaded with rhBMP-2.
The content of collagen in the CBCP in the present study was 4-7% (by volume). Given that the addition of this small amount of collagen increased the mean area of new bone and favorably affected the bone healing pattern, using a larger volume of collagen in CBCP may alter the effect of rhBMP-2. In a pilot study, Yun et al. [21] recently compared the CBCPs containing 4-7% and 47% collagen (by volume). In that study, the CBCP with the lower collagen content resulted in more new bone formation than that with the higher collagen content; the volume stability of the latter may have been impaired due to collagen comprising almost half of its volume. From a clinical viewpoint, an increased collagen content may enhance the clinical manageability of the carrier due to the concomitant increase in tensile and shear strengths. Thus, determining the optimal balance between the regenerative capacity and clinical manageability of carriers, in terms of the ratio of collagen content, requires further study.
Collagenated bone substitutes including CBCP in the present study have received attention for several indications, such as ridge preservation, lateral onlay grafting, periodontal regeneration, and sinus augmentation. They offer improved clinical manageability in unfavorable types of defect, preventing scattering of graft particles and providing moldability to fit the specific defect morphology. Bovine HA incorporated with collagen matrix was found to be easily fixed to the lateral surface of the canine maxilla [2], and CBCP was shown to be useful for the vertical augmentation of rabbit calvaria [16]. When loaded with rhBMP-2, the three-dimensionally prefabricated porous structure of these carriers provides a favorable environment for new bone formation and angiogenesis [24].
The term “optimal” can be defined as “providing efficacy with a small dose” in regard to rhBMP-2 application. However, clinical situations and carrier materials should be taken into consideration for this optimization. Within the limitations of the present study, 0.005 mg of rhBMP-2 could improve bone regeneration at an early healing period when loaded on BCP and CBCP in the rabbit calvarium. Different healing patterns of CBCP, such as more new bone formation along the intergranular space at an early healing period may give additional benefits together with easy clinical manageability. Future studies should be performed to confirm those findings in a larger number of animals and in different models.






 XML Download
XML Download