

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The sealing ability of the peri-implant nonkeratinized tissue [1] and the critical role of bacterial plaque control in some patients are the main arguments for justifying a gingival graft at the implant site [2]. Several clinical and experimental investigations have shown that the absence of the attached keratinized tissue is compatible with the maintenance of periodontal health [3]. Furthermore, some authors have reported no correlation between the implant success rate and the presence of keratinized tissue in the peri-implant soft tissue [4,5,6]. On the other hand, some reports have suggested that a lack of keratinized tissue contributes to implant failure and that mobile mucosa can disrupt the implant-epithelial attachment zone and contribute to an increased risk of inflammation due to the accumulation of plaque [7,8,9,10,11,12].
However, there is a lack of consensus in the literature regarding the relationship between the width of the keratinized tissue and the health of peri-implant tissues [13,14,15]. Nevertheless, it is generally accepted that a more ideal and healthy soft tissue-implant interface can be established if an adequate zone of keratinized tissue is present [16,17], based on the rationale of enhanced esthetics, easier restorative manipulation, less gingival recession, easier plaque control, and regular maintenance care [18,19,20].
Various surgical techniques have been used to obtain adequate amounts of keratinized tissue around dental implants, including the gingival autograft, apically positioned flap (APF), coronally positioned palatal sliding flap, and acellular dermal matrix graft (ADM) [21,22,23,24]. Performing a free gingival graft (FGG) prior to implant surgery has been suggested when there is minimal keratinized tissue over the edentulous ridge [25,26], and APF and FGG can be combined in shallow vestibules with minimal keratinized tissue [27].
These procedures are usually performed before implant placement or during the exposure of submerged implants, which can extend the healing period and result in patients suffering from pain and discomfort through several surgical stages. In addition, these can be time-consuming procedures in cases that already have good primary implant stability and do not need hard-tissue augmentation.
Here, we describe an interpositional gingival graft technique that is performed at the time of implant placement. The graft consists of two parts-an epithelium-connective tissue (E-C) portion and a connective-tissue-only (CT) portion-and is partially inserted under the buccal flap. The aims of this case report are to describe a simultaneous interpositional FGG (iFGG) procedure with the placement of nonsubmerged implants in a patient lacking keratinized tissue, and to report the findings of our assessment of the long-term outcome of this grafted tissue.
CASE DESCRIPTION
Patient information and site analysis
A 50-year-old female patient presented to the Department of Periodontology at Yonsei University Dental Hospital, Seoul, Korea, complaining of partial edentulism in the right mandible. The patient had no contributing medical history. The mandibular right second premolar and molars had been extracted 10 years previously, and she had been wearing a removable partial denture.
The posterior molar site of the edentulous mandible presented a thin band (approximately 2 mm) of keratinized tissue on the ridge crest and inadequate vestibular depth (Fig. 1). The treatment plan included the placement of three nonsubmerged implants in the positions of the mandibular right second premolar, first molar, and second molar. In addition, simultaneous interpositional free gingival grafting was planned in the molar area to increase the amount of keratinized tissue.
The protocol was reviewed and approved by the Yonsei University Institutional Review Board. The patient provided written informed consent before the onset of the surgery.
Surgical procedure
Recipient site preparation and implant placement
A horizontal incision was made on the ridge crest starting from the distal gingiva of the first premolar and extending to the posterior area (Fig. 2). The horizontal incision line of the molar area was on the mucogingival junction. Thus, the lingual flap had 2 mm of keratinized tissue. Full-thickness buccal and lingual flaps were elevated, and the keratinized tissue band of the molar area was then repositioned to the lingual flap. Nonsubmerged implants (Standard implant, Straumann, Basel, Switzerland; second premolar and first molar: diameter 4.1 mm, length 12 mm; second molar: diameter 4.1 mm, length 10 mm) were placed, and healing caps (diameter 6.5 mm, height 1.5 mm) were connected following a standardized technique.
Donor site preparation
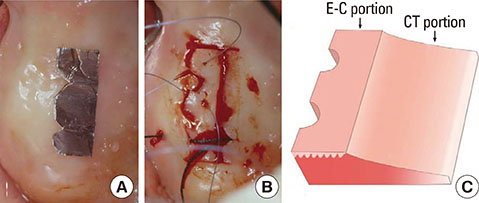
The right palate was chosen as the donor site. The thickness of the palatal tissue, as measured by penetrating to the bone with a periodontal probe, was approximately 3.0 mm. A tinfoil template was used to guide the palatal incision (approximately 7 mm high and 20-mm wide). The graft contouring was performed with a fresh No. 15C scalpel to ensure close adaptation around the implant abutment and a butt-joint marginal adaptation with the lingual tissues. A presuture for the sling suture was made to adapt and fix the graft immediately, and a partial-thickness graft was harvested (Fig. 3A and B).
Fixation of the graft and postoperative care
The graft was positioned over the recipient bed, and the CT portion was inserted under the buccal flap and sutured to the buccal mucosa flap to promptly obtain a blood supply from the buccal flap and the underlying bone tissue. The presutured silk on the E-C portion was tied around the healing caps using sling sutures. The graft was then closely connected to the lingual flap by using an interrupted suture to obtain primary closure in the interproximal area. Consequently, the buccal flap was positioned apically and fixed at the inferior border level of the E-C portion (Fig. 4).
Light compression was applied to the graft with moistened gauze for about 5 minutes to reduce the thickness of the blood clot and enhance fibrin adhesion. All surgical procedures were performed by one of the authors (K.S.C.).
Postoperatively, the patient was instructed to rinse her mouth twice a day with 0.1% chlorhexidine solution (Hexamedine, Bukwang Pharmaceuticals, Seoul, Korea) for the first 2 weeks after the surgery. Antibiotic regimens were prescribed for 7 days, and the sutures were removed after 10 days. The patient was rehabilitated with a fixed partial denture after 4 months.
Healing and analysis
The healing was uneventful during the initial healing period, and the graft appeared well integrated with the surrounding tissues. The patient was seen at 2, 4, 6, 8, 16, and 20 weeks postoperatively, and yearly thereafter for 8 years to monitor healing and for plaque control. Clinical and radiographic examinations were carried out once or twice a year (Figs. 5 and 6). Plaque control and oral hygiene reinforcement were performed at each visit.
A clinical examination performed 8 years after surgery found no significant signs or symptoms of inflammation, such as bleeding on probing, gingival redness, or swelling on the keratinized tissue around the implants, and increased keratinized tissue by the creeping attachment was observed. The grafted gingiva had been well maintained throughout the healing period. Table 1 lists the changes in the width of the keratinized tissue after specific periods of healing. The width of keratinized buccal gingiva had increased to 4 mm, and the buccal vestibule was deeper than in the preoperative condition.
DISCUSSION
In the presented case, iFGG was performed simultaneously at the time of implant placement to increase the amount of keratinized tissue around the implants. The presented graft technique was modeled on the "interpositional onlay graft" technique developed by Seibert and Louis [28], and retained the advantages of their technique. The interpositional onlay graft was originally developed for treating large class-III ridge defects. Interpositional grafts can receive their new blood supply from the connective tissue bed and provide buccolingual ridge augmentation. Onlay grafts were designed primarily to achieve apicocoronal ridge augmentation. The interpositional onlay graft was meant to combine the advantages of the interpositional graft and the onlay graft into a single procedure.
In the present case, the graft was positioned over the recipient bed and the CT portion was inserted under the buccal flap. The expected healing was more rapid and favorable at the recipient site. This feature might have also helped to prevent the postoperative shrinkage of the grafted gingiva; there was no conspicuous shrinkage of the grafted gingiva in this case. It is presumed that the buccal flap and the recipient bed provided a copious blood supply and that the graft itself was sufficiently wide.
Vertical shrinkage of FGGs is a well-known clinical phenomenon that occurs mainly during healing in the first postoperative year, with an average of 42.3% shrinkage reported in thin grafts [29] Orsini et al. [30] investigated the dimensional changes of FGGs for 1 year after surgery. Average vertical shrinkages of 10.2%, 28.4%, 37.2%, and 43.5% were identified after 1, 4, 26, and 52 weeks, respectively. The width of the keratinized buccal gingiva in the present case had increased to 4.5 mm at the site of the first molar. In addition, the buccal vestibule had deepened and the mucogingival junction had shifted apically. The results were favorable and stable compared with those of other studies using FGGs, APFs, or ADMs. Barone et al. [31] found that the width of the masticatory mucosa at 12 months after FGG prior to implant surgery was 3.7±1.0 mm (mean±standard deviation), and was 3.2±0.9 mm after APF with second-stage surgery. Park [32] demonstrated that the use of an ADM increased the width of the peri-implant keratinized mucosa from 0.8±0.6 mm to 3.2±0.9 mm at 3 months and 2.2±0.6 mm at 6 months.
Interestingly, the gingival margin of the first molar implant in this case had coronally shifted 8 years postoperatively compared with 1 year postoperatively. This shift was associated with a slight increase in the thickness of the keratinized tissue compared to the baseline. The probing depth increased to 4 mm, but there was no sign of inflammation (such as bleeding) on probing. There is no report in the literature of a postoperative "coronal" migration of the gingival tissue around implants. A controlled trial of this surgical protocol is needed to elucidate the precise changes in the soft tissue that occur around implants during the healing period.
The long-term clinical and radiographic observations presented here suggest that this surgical protocol provides several clinical benefits over other techniques for increasing the amount of keratinized tissue, such as deepening of the buccal vestibule, rapid revascularization of the grafted gingiva, shortening of the healing time, and prevention of graft shrinkage. The use of simultaneous iFGG with the placement of an implant could minimize the number of surgical stages required and thus, the level of patient discomfort, while predictably providing an adequate zone of buccal keratinized tissue. Therefore, the technique may be considered an alternative method for increasing the amount of keratinized tissue for cases that have a minimal amount of keratinized tissue around implants.







 XML Download
XML Download