

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since Brånemark introduced a protocol for dental implantation in 1977, implants have become increasingly successful in the restoration of the dentition of partially or completely edentulous patients [1-3]. In addition, root-form endosseous dental implants have proven to be excellent alternatives to conventional tooth replacement options [4]. Achieving good primary (biomechanical) stability is a prerequisite for successful implantation [5]. This depends on many factors, including the implant design and surface, bone quality, and implantation procedure [6,7]. During the last 20 years, implant designs and surfaces have been developed to achieve faster and more stable osseointegration and higher success rates. Though the original Brånemark implant system had smooth endosseal surfaces, the currently marketed rough endosseal surfaces deliver higher success rates, especially in areas of cancellous bone quality [8,9]. Among the various rough surfaces, the sand-blasted, thermally acid-etched surface encourages more rapid implant osseointegration, thereby shortening the healing period, and it has the potential to become the gold standard soon.
Such an implant system, characterized by a sand-blasted, thermally acid-etched surface, machined collar, and internal hexagonal implant/abutment connection, was introduced in 2001. The implants are threaded, self-tapping, and have either cylindrical (constant diameter) or conical-cylindrical endosseous profiles. They have a tapered and domed apical end that promotes smooth insertion into the implant bed. The state-of-the-art manufacturing process results in an optimal implant surface and the self-tapping design contributes to achieving good primary stability.
Although entailing many advantages, these implants are newer than other brands and their use in clinical practice has not been documented for a prolonged time period; that is, the literature provides scant survival rate analysis. As these implants share many characteristics with currently used implant brands, a survival rate study of this implant line could provide the proof that its reliability and predictability is also comparable to competitor products. The goal of this study was thus to evaluate the medium-term survival rate of this implant system.
MATERIALS AND METHODS
A retrospective chart review was conducted with the aim of evaluating the survival rate of a newly introduced implant line. Two university clinical centers have participated in the review. Both clinics have collected ample experience with these implants. Kyung Hee University Dental Hospital provided information from 140 patient charts comprising 262 implants, while Myong Ji Hospital contributed 41 patient charts with 90 implants. The protocol of this study, which used anonymized patient data, imposed no additional risk to the patients who were included and involved no procedures for which written informed consent was needed. It was approved by the Institutional Review Board (IRB) at the Dental Hospital of Kyung Hee University (KHD IRB-004-1), and the chart review was conducted according to the Declaration of Helsinki.
The 352 implants analyzed in this study were used for treatment of single or multiple tooth loss. The implants were manufactured of pure titanium (grade 4). They had either a cylindrical (SPI ELEMENT and SPI ONETIME, Thommen Medical AG, Waldenburg, Switzerland) or a conical-cylindrical design (SPI CONTACT, Thommen Medical AG). All of the implants are included in this report; in other words, no patient was excluded from the analysis population. All of the implants were inserted following standard surgical protocols. Care was taken to ensure the ideal prosthodontic implant position and that the implant sites had the appropriate bone quality and bone volume.
The placement of the implants was performed according to the manufacturer's recommendations, after raising a muco-periosteal flap. The implants were allowed to heal either submerged or non-submerged. Permanent prosthetic rehabilitation was scheduled after a healing time of 6 months.
The statistical analysis was performed using Cutler and Ederer's life table method for survival analysis. The principal advantage of this method is that it enables the use of all survival information gathered up to the closing date of the study. Thus, the implants that entered observation 4, 3, 2, and even one year prior to the closing date also contributed useful information to the calculation of the 4-year survival [10].
RESULTS
Patient characteristics
The age distribution of the patients in the study together with the corresponding implant breakdown is shown in Table 1. The average patient age at the time of implant insertion was 55.2 years (19 to 87 years). A total of 352 implants was inserted in this patient population between July 2006 and March 2009. 104 of the patients (57.5%) were male and 77 (42.5%) female. The largest group age group was 50-59 years, both in terms of the number of patients (64 patients, 36.8%) as well as the number of implants (136, 38.6%). In addition to systemic diseases, including hypertension, diabetes, angina pectoris, asthma, hyperthyroidism, hyperlipidemia, and tachycardia were seen in 61 patients (32.1%). 39 patients (11.1%) were smokers, thus reflecting the general patient population in Korea.
Implant distribution
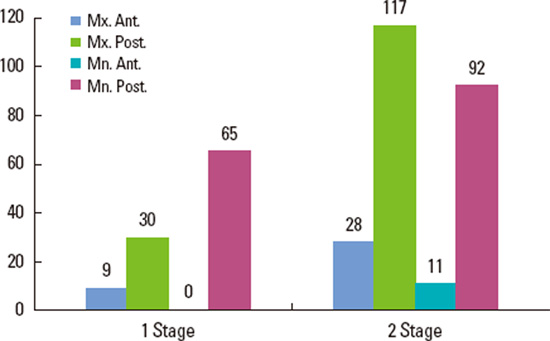
Table 2 shows the positions of the reported implants. 184 of the implants (52.3%) were placed in the maxilla. Among these, 37 (10.5%) were placed in the anterior and 147 (41.8%) in the posterior regions. One hundred sixty-eight implants (47.7%) were placed in the mandible, with 11 (3.1%) in the anterior and 157 (44.6%) in the posterior region.
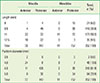
The distribution of the implant length and diameter is shown in Table 3. The length ranged from 8 to 12.5 mm. 21 of the implants (6.0%) were 8 mm long and 35 (9.9%) were 12.5 mm long; that is, the majority of the implants were either 9.5 mm (n=119, 33.8%) or 11 mm (n=177, 50.3%) long. The implant platform diameter ranged from 2.7 to 5 mm. Only a few implants (n=2, 0.6%) had a reduced diameter (platform, 3.5 mm); most of the inserted implants had a 4.5-mm platform diameter (n=218, 61.9%). The majority of the implants were inserted into bone with quality of types II and III (n=316, 89.7%) [11]. The bone quantity was classified as B and C (n=307, 87.2%) (Table 4).
Surgical protocols and prosthetics
The implants were placed using both nonsubmerged (1 stage) and submerged (2 stage) surgical protocols (Fig. 1). Fig. 2 summarizes the restoration types: single crowns (n=249, 70.7%), bridges (n=101, 28.7%), or full dentures (n=2, 0.6%). As shown in Table 5, 212 implants (60.2%) were placed in sites with bone grafting procedures, such as crestal or lateral sinus floor elevation, guided bone regeneration, ridge expansion, etc.
Implant survival
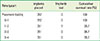
Implant survival was evaluated using the criteria of Albrektsson and Zarb [12]; specifically, implants still stable in situ were considered to be survivors. During the follow-up period, only one of the 352 implants was lost. This implant (platform diameter, 4.5 mm; length, 9.5 mm), was inserted into the mandible. It had to be removed due to osteomyelitis approximately 21 months after loading. 3 months following implant removal, the site healed uneventfully. Using the above-mentioned criteria for implant survival, the life table analysis resulted in a cumulative survival rate of 99.7% (Table 6).
DISCUSSION
Only a few of the currently marketed dental implant systems have documented mid- or long-term survival rates. When a new, substantially equivalent implant system is brought to market, current regulations do not require prospective clinical trials to determine the predictability of the specific system. An efficient option to achieve this is thus a retrospective chart review study. One of the advantages of such a review is that its result is a true reflection of general clinical practice with the system in question. The purpose of this study was to evaluate the medium-term (4-year) survival rate of 352 implants from a newly introduced titanium implant line. The results reported here were obtained in 181 patients in two independent clinics. The 99.7% cumulative survival rate is the result of only one failure in the investigated timeframe. This clearly indicates that the implants have still been present and stable in situ after the four year period studied. In addition, no severe complications, such as pain or mobility, were recorded in the 4-year period.
With other titanium implant lines, several prospective studies have been already published that document their survival rate. These systems might differ somewhat in their endosseal surfaces and designs. A survival rate of 92.6% has been reported, for instance, for Brånemark implants, after 10 years of follow-up [3], while for another implant line with a titanium plasma-sprayed surface, a 96.7% 8-year cumulative survival rate was reported [13]. Recently, root-shaped implants with sand-blasted, thermally acidetched surfaces showed a cumulative survival rate of 98.6% to 99.3% [14,15]. The results of the present retrospective multicenter chart review study comprise a total of 352 state-of-the art titanium implants placed in 181 patients. The results showed quite a high four-year survival rate of 99.7%. Our findings, therefore, showed that the tested implants provide a safe and predictable clinical outcome that compares well with other implants for which the survival rates have been published earlier.
The single implant lost was due to osteomyelitis. At the time of implant placement in the right posterior mandible, the female patient was 79 years old. After a 5-month healing period, prosthetic treatment was initiated. Some 21 months after the implant placement, the patient presented at the clinic with gingival swelling and pain in the implant area. Radiographic findings had confirmed osteomyelitis and a sequestrectomy with removal of the implant and the adjacent tooth was performed under general anesthesia. The patient recovered uneventfully.
It should be noted that a large number of implants, that is, more than half of the implants reviewed in this study, were placed in areas requiring additional interventions such as sinus floor elevation or guided bone regeneration due to poor bone quantity and/or quality at the implant site. Consequently, the majority of the cases can be classified as complex. Considering this background, the finding of only 1 failed implant among the 352 cases after 4 years is quite impressive. The implants that were used represent a very reliable alternative when a substitution for natural teeth is required.
The tested implants feature a sand-blasted, thermally acid-etched endosseous surface. The roughness value, Sa, is 1.0-2.0 µm. This surface is therefore classified as moderately rough. The advantage of moderately rough surfaces is that they show stronger bone responses than smoother or rougher surfaces, and contribute to achieving a favorable clinical performance [16]. Further advances in surface processing (conditioning with a week base) created a hydrophilic surface, which is known to accelerate the healing process by promoting the activity of osteoblasts, the bone-forming cells that play a key role in the integration of implants into bone [17]. The results from mechanical and histomorphometric analyses in animal studies have shown a significantly higher removal torque and percentage of bone-to-implant contact for rough surfaces when compared to machined surfaces [18,19]. A human histology study demonstrated that the rough surface developed a statistically higher percentage of bone-to-implant contact than the machined surface [20]. This implant system also provides different designs for the machined collar height. The availability of such an array of sizes enables the practitioner to select the fixture with an optimal design to ensure a successful treatment outcome. Depending on the requirements of the particular implantation site, as well as the condition of the surgical site and additional surgical demands, the optimal implant can be effectively selected. The present retrospective study focused on the 4 year cumulative survival rate. A longer-term follow-up study and comparison with other implant lines (with different surface structures and geometry) would be feasible.
The cumulative survival rate of 352 titanium implants was determined to be 99.7% after four years. This calculation was based on a retrospective evaluation of implant survival. The availability of the assessment of other clinical parameters, mainly periodic radiographs, would have allowed the calculation of implant success to further support the outcome achieved with the tested implant line. Within the limitations of this retrospective chart review, we conclude that the newly introduced implant system is a safe and predictable option for restoring partially or completely edentulous patients and also in cases when additional bone grafting procedures are needed.



 XML Download
XML Download