

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Elevation of the maxillary sinus floor before implant placement may be necessary when the bone height of the posterior maxilla is insufficient [1,2]. Maxillary sinus floor augmentation can be achieved by a crestal or lateral approach, but when the residual alveolar bone height (RBH) is insufficient, the lateral window approach is the preferred method. When performing maxillary sinus floor augmentation, the risk of complications must be considered and foreseen [3]. One of the complications reported during surgery is excessive bleeding from the bony window [4], which occurs when a small artery that supplies the sinus is severed. Because of the reactive contraction of the cut vessels, transection of the artery is not life-threatening [5], but visualization of the Schneiderian membrane may be impaired, making the membrane elevation far more difficult and interfering with the placement of the graft materials [6]. The lateral maxilla is supplied by branches of the posterior superior alveolar artery (PSAA), also known as the alveolar antral artery [5,7] and the infraorbital artery (IOA); these arteries form an anastomosis in the bony anterolateral wall, which also supplies the Schneiderian membrane [8].
To avoid severing these arteries, it is important to anticipate the location of the anastomosis during bony window preparation. Earlier reports on the location of this anastomosis have been based mostly on cadaver studies [8,9] or radiographic studies [10,11,12]. Most previous studies measured the distance from the alveolar ridge crest to the anastomosis; however, progressive atrophy of the alveolar ridge with age and tooth loss results in changes to the position of the crest, which complicates the implant placement [13]. Only a few studies have investigated the intraosseous anastomosis location with respect to the tooth position and the position of the maxillary sinus floor [14,15].
Computed tomography (CT) and cone-beam computed tomography (CBCT), which provide sectional views, are used for dental implant installation procedures, particularly in areas with anatomical limitations [16,17,18]. CT and CBCT are considered more accurate than intraoral or extraoral radiography and can provide 3-dimensional information about maxillary sinus structures [19,20,21]. Hence, our aims in this study were first, to measure the distance of the intraosseous anastomosis in the anterolateral wall of the maxillary sinus from different reference points, and second, to correlate the location of the intraosseous anastomosis with the residual bone height of the maxilla and the tooth positions obtained using CT scans.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board for Clinical Research at Samsung Medical Centre (IRB No. 2010-02-002). We collected information from 283 patients scheduled for implant-supported restorations in the posterior edentulous maxilla. Of these 283 patients, 186 were men and 97 were women, ranging in age from 18 to 84 years (mean, 57.1 years). CT images were obtained using a GE LightSpeed VCT (General Electric Medical Systems, Milwaukee, WI, USA) with an 18- to 20-cm field of view operated at 120 kV and 300 mA. The scanning time was 4-6 seconds, the rotation time was 0.6 second, and the slice thickness was 0.625 mm [21]. After the CT images were obtained, they were analyzed using a specialized software program (10DR Co., Seoul, Korea).
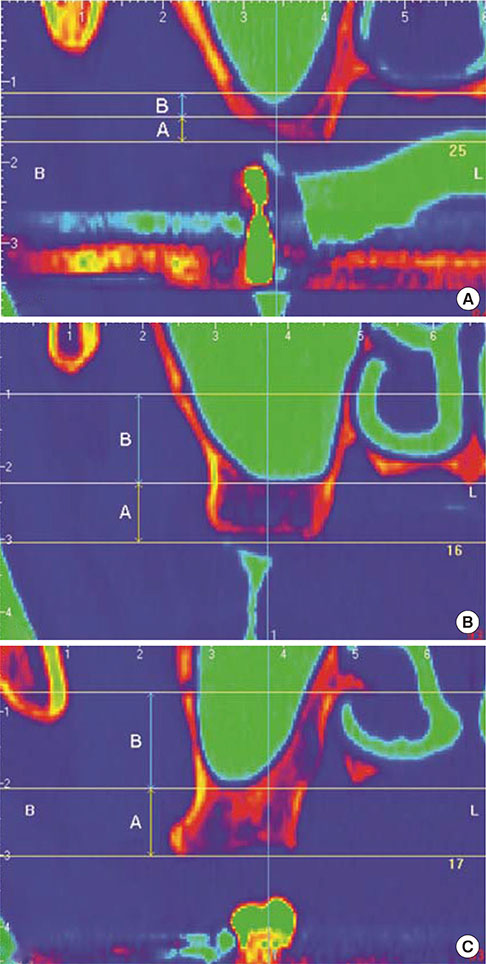
The anastomosis of the PSAA and the IOA was located, and the distances from the anastomosis at the edentulous sites from the first premolar to the second molar area were measured in 283 patients. Radiographic CT stents were made considering the tooth position and the occlusal relationship. All patients had radiographic stents placed before undergoing CT, and the central section of each designated tooth in the edentulous area was chosen for measurement. To ensure accurate measurements, the CT images were magnified to five times their original size. The images were colorized to simplify the evaluation of the hard and soft tissue interface (Fig. 1). Irrespective of the amount of resorbed alveolar bone crest, the RBH was measured from the ridge crest to the lowest point of the maxillary sinus floor and then, categorized by distance: less than 4 mm (group 1), between 4 and 8 mm (group 2), and greater than 8 mm (group 3). The distance of the anastomosis position from the ridge crest was measured as follows: Three horizontal lines were drawn at the ridge crest, the maxillary sinus floor, and the position of the anastomosis. A vertical second line at the center of each tooth was drawn perpendicular to the horizontal lines. The distance from the ridge crest to the maxillary sinus floor (A) and the distance from the maxillary sinus floor to the bony canal (B) were measured from the intersections of the horizontal and vertical lines (Fig. 1). All measurements were performed with 10DR implant software by two trained examiners.
All measurements were expressed as mean±standard deviation. In this study, we collected data from tooth positions at the left or right side of maxillary sinuses in each patient and regarded our data as the correlated data of the patients because the observations measured on the left or right side of each tooth position from each patient were correlated. Therefore, we applied a linear mixed model with the adjustment of the side of each tooth for the hypotheses of interest. Statistical analyses, including a linear mixed model with Bonferroni correction and post hoc tests to compare the difference between groups or teeth, were performed using SAS 9.3.1 (SAS Institute, Cary, NC, USA). The difference in the location of the anastomosis from the residual alveolar ridge crest or the maxillary sinus floor between sexes was also compared using a linear mixed model with a Bonferroni correction. A P-value less than 0.05 was was considered statistically significant.
RESULTS
The anastomosis between the PSAA and the IOA was discernible in 92 out of 283 patients (32.5%). The mean distance from the alveolar ridge crest to the intraosseous vascular anastomosis (IVA) at each tooth position was 19.6±5.64 mm at the first premolar (P1), 19.9±5.87 mm at the second premolar (P2), 15.6±4.06 mm at the first molar (M1), and 16.5±4.75 mm at the second molar (M2) site (Table 1).
In this study, there were only 6 images at the first premolar site; therefore, for the P1 site, only the measurements were described. The number of sites for the statistical analysis of the second premolar, first molar, and second molar groups was sufficient (Table 1). The residual alveolar ridge heights (RBHs) of different tooth types were significantly different (P=0.0002). The RBH at P2 is greater than that of M1 (P=0.0002) and M2 (P=0.0018). There was no statistical difference in the distance from the sinus floor to the IVA position according to the teeth position (Table 1). The distance of the IVA position from the alveolar ridge crest equals the sum of RBH and the distance from the maxillary sinus floor to the IVA. Therefore, the distances from the alveolar ridge crest to the IVA between P2 and M1 (P=0.0003) and between P2 and M2 (P=0.0018) were statistically different (Table 1). The relationship between the RBH and the IVA from the maxillary sinus floor is shown in Table 2. When analyzed with a post hoc test, there were significant differences between groups 1 and 3 (P=0.0039). The distance from the maxillary sinus floor to the IVA was the smallest in group 3. The correlation between the RBH and IVA from the maxillary sinus floor according to the tooth position is shown in Fig. 2 and Table 3. At the P2 site, there was no correlation between RBH and the distance from the maxillary sinus floor to the IVA. However, at the molar sites, there was a moderate negative correlation and the regression coefficient was -0.4788 and -0.5772 at M1 and M2. The distance among the alveolar ridge crest, maxillary sinus, and the IVA position was not statistically different between the sexes (Table 4). It was not possible to perform a statistical analysis for the first premolar site due to an insufficient sample size (only one female). Therefore, no first premolar site was included in group 1 (Table 3).
DISCUSSION
An anastomosis between the PSAA and the IOA in the sinus anterolateral wall was found in 100% of the cases by cadaver dissection [5,6,8,9], while the bony canal was identified in 47%-55% of cases with CT images [6,10,12,22]. With CT images, it is difficult to identify anastomoses that have a very small diameter [22] or when they travel along the sinus membrane. In this study, we found well-defined bony canals in 32.5% of the patients. This is a relatively low proportion compared with previously published results [6,10,12]. This result may be partly due to the shape of the anastomosis. 61% of the bony canals identified in this study were partially covered with bone and could easily be missed. Another possibility for a relatively low proportion found radiographically is the diameter of the bony canal. Vessels less than 0.5 mm in diameter could not be identified with CT scans in most of the cases [22] although the diameter of the vessels was not measured in this study.
We found that the average distance from the residual alveolar ridge crest to the intraosseous anastomosis was 18.3 mm (data were not shown); this is in accordance with earlier studies that reported that the anastomosis between the PSAA and the IOA was located at an average distance of 18.0 mm [11] and 18.9 mm [8] from the alveolar crest of the posterior maxilla. However, other studies [6,10,12] reported a shorter mean distance, which ranges from 11.25 to 16.9 mm, than that of our study. Previous research [6] mentioned that such data could be misleading because the height of the residual bony ridge, the maxillary atrophy class, and the presence of teeth play a relevant role in determining the location of the vessel. In this study, we used both the residual bony ridge and the maxillary sinus floor as reference points for measuring the intraosseous anastomosis position (Table 1). From the residual alveolar bone crest, the mean distance to the intraosseous anastomosis was the greatest at the first premolar tooth with 21.0±5.41 mm and the shortest at the first molar tooth with 15.6±4.06 mm although there were only limited data for P1 sites. Our findings were in accordance with recent papers [12,15], which showed that the mean distance from the alveolar crest and the sinus floor to intraosseous anastomosis is related to the tooth position. The course of the bony canal is curved, with the most inferior site in the first molar tooth position; this agrees with the anatomic studies of other researchers (Table 1) [8,9]. The maxillary sinus floor resembled the course of the vessel, lowest in the first molar and highest in the first premolar area of edentulous patients [15]. However, in a dentate cadaver study, although a slight height increase from the first molar to the first premolar regions existed, the sinus floor height variation according to the tooth position was minimal [14]. In this study, the mean distance from the maxillary sinus floor to the intraosseous anastomosis position was not significantly different among different tooth positions; this agrees with the results from the study on dentate cadavers, although in our study, the sample size for the P2 site was relatively small (Table 1).
A few studies have described the relationship between the intraosseous anastomosis position and the remaining alveolar bony height [11,12]. These previous studies used the descriptive definition of the jaw shape from Lekholm [23], but we decided to classify groups according to the remaining alveolar bone height. Our study divided the height of the residual bony ridge into 3 groups to investigate the distance from the maxillary sinus floor to the intraosseous anastomosis. According to the results of this study, the higher the residual bony ridge is, the shorter is the distance from the maxillary sinus floor to the intraosseous anastomosis (Table 2). However, when we evaluated the correlation between the distance from the maxillary sinus floor to the intraosseous anastomosis and the RBH at each tooth position, there was a correlation only in the case of the molar teeth (Table 3). We found a moderate negative correlation between the RBH and the distance from the maxillary sinus floor to the intraosseous anastomosis position. We also found that the greater the RBH is, the shorter is the distance from the maxillary sinus floor to the intraosseous anastomosis in the case of the molar teeth (Table 3).
Other studies [10,15,24] reported that 20%-31% of arteries were located less than 15 mm from the alveolar crest. Therefore, it is recommended that the bony window should be planned to be elevated no higher than 15 mm above the alveolar crest [15]. The location of the bony window for a lateral augmentation of the maxillary sinus is dependent on the height of the residual alveolar ridge, the length of the implant to be placed, and the position of vascular anastomosis. On the basis of the results of this study, we can conclude that a greater height of the residual alveolar ridge and a higher position of the bony canal do not mean a higher risk of severing the artery during the window preparation in the P2 site; however, in the molar regions, sites with a greater remaining alveolar ridge height have a relative high risk during the window osteotomy preparation due to the correlation between the RBH and the distance from the maxillary sinus floor to the intraosseous anastomosis position.
There was no statistically significant difference between teeth positions and between sexes with respect to the distance from the maxillary sinus to the bony canal position; this is in accordance with previous findings [14]. They found that the height of the bony canal reference to the maxillary sinus floor is more reliable than the use of the residual bony ridge in dentate cadavers. Therefore, measuring the distance from the alveolar crest to the intraosseous anastomosis would not help in designing osteotomy windows for a sinus grafting procedure to place longer implants in the resorbed posterior maxilla. Our previous paper reported that the lateral wall of the sinus was thinner in women [21]. It would thus be prudent to pay attention to the thickness of the lateral wall of the maxillary sinus in window osteotomy preparation in women instead of the intraosseous anastomosis position from the alveolar ridge crest or the maxillary sinus floor.
In this study, the tooth position was approximated from the radiographic CT stents used. However, with this method, the amount of ridge resorption could not be measured at each tooth position. The distance from the alveolar bone crest and the maxillary sinus floor to the intraosseous anastomosis in an edentulous patient (Table 1) is smaller than that of the dentate cadaver [14]. Further research is needed that would include the amount of ridge resorption as a variable to predict the position of the intraosseous anastomosis of the PSAA and the IOA. The findings of this study will help enable clinicians to perform safe osteotomy window preparation.




 XML Download
XML Download