

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
According to the reports of the National Health and Nutrition Examination Survey (NHANES III, 1988-1994) in the United States [1], gingival recession defects, characterized by the exposure of the tooth root surface and the symptom of dentinal hypersensitivity, affected more than 50% of the population. To resolve these complications, covering the tooth root with the gingival tissue by performing periodontal plastic surgery, namely the 'root coverage' procedure, was proposed. The coronally advanced flap (CAF) and laterally positioned flap (LPF) were the two main techniques used in this root coverage procedure [2]. These techniques, combined with the use of tissue grafts or biomaterials, were proposed to increase the predictability of clinical outcomes by providing extra tissue, increasing flap thickness, and guiding tissue growth [3,4].
CAF has been widely used for treating gingival recession for fifty years now [5], and there is plenty of clinical evidence supporting the predictability of CAF or CAF combined with a tissue graft [4]. The LPF, also called the sliding flap, lateral pedicle flap, or rotated flap, was first introduced by Grupe and Warren Jr [6] in 1956, and either combination with [7,8] or without subepithelial connective tissue graft (SCTG) placement under specific circumstances was suggested [9,10,11]. The combination of LPF and SCTG can improve root coverage, reduce the chances of gingival recession of the flap elevation site [12], and retain the advantages of the LPF technique, such as flap flexibility and obtaining predictable keratinized gingiva [13].
Of all the root coverage procedures, CAF combined with SCTG is the most commonly used one and is regarded as the most predictable technique for Miller class I or II gingival recession defects [2,3,4] (Miller's classification) [14]. However, the therapeutic effect of this procedure on advanced cases, such as Miller class III gingival recession with a wide and deep defect, is still inconclusive. Although acceptable clinical results for treating Miller class III cases by using CAF+SCTG have been reported, most of these cases originally had just mild interproximal bone loss and minor-to-moderate gingival recession defects [15]. On the other hand, although LPF was not investigated quite as often as CAF, the clinical outcomes of these two procedures were comparable [4]. In certain clinical circumstances, such as the limited amount of keratinized tissue apical to the recession defect and presence of a very shallow vestibule, LPF can be an alternative to CAF to obtain predictable root coverage [12].
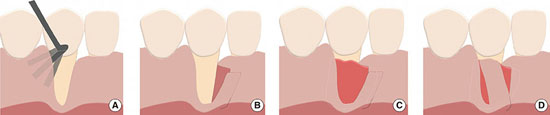
The three cases with advanced gingival recession discussed in this report were treated with a modified laterally positioned flap (mLPF), characterized by an oblique incision beyond the mucogingival junction with a partial thickness flap to increase the flap flexibility (Fig. 1A, B). SCTG was placed to augment tissue thickness and obtain predictable biological attachment, thereby increasing the root coverage rate (Fig. 1C, D) [4]. All patients were treated in the periodontal clinic of the College of Dental Medicine, Columbia University. The percentage of root coverage as well as self-reported hypersensitivity before and after surgery was assessed, and the results are summarized in Table 1.
CASE DESCRIPTION
Case I
History
A 50-year-old female, who had undergone orthodontic treatment in private practice in 2007, presented with generalized severe root resorption and buccal gingival recession (Fig. 2A, B), which caused esthetic concerns and root hypersensitivity, in a consultation appointment. The gingiva of the mandibular right canine was inflamed, with insufficient width of the keratinized gingiva. The mandibular right canine exhibited significant root prominence and a Miller class III gingival recession defect (Fig. 2B). The tooth was vital as determined by a cold test and grade I mobility [16]. The patient was informed that the tooth had questionable prognosis due to severe periodontal attachment loss. Further, complete root coverage could not be expected due to the significant interproximal bone loss.
Treatment and outcome
The exposed root surface of the mandibular right canine was scaled and root planed before flap elevation, and no chemical reagent or drug was utilized to condition or clean the root surface. The distal interproximal gingiva was partially elevated by using the tunneling technique [17], and the mesial interproximal gingiva of the mandibular right canine was included in the mLPF. Vertical and oblique incisions were made (Fig. 2C), and then, a split thickness flap was elevated. After flap elevation, the mandibular right canine revealed a significant loss of the buccal alveolar bone and severe root resorption (Fig. 2D). SCTG was harvested from the palate by using the two-incision flap design. The selection of the size of tissue graft (dimensions: 16 mm×8 mm×2 mm) was based on the areas of the recession defect and flap elevation sites. The graft, whose position was 1 mm below the cementoenamel junction (CEJ) level and 3 mm above the interproximal bone level, was placed underneath the mesial and distal interproximal gingiva. Stabilization of the tissue graft was achieved with a chromic gut 5-0 suture. The split thickness flap was distally rotated to cover the exposed tissue graft and was sutured with chromic gut 5-0 (Fig. 2E). The patient was instructed to take ibuprofen 800 mg every eight hours as needed for resolving postoperative pain or discomfort, and rinse the mouth for 30 seconds twice a day with half an ounce of 0.12% chlorhexidine to maintain the hygiene of the surgical area during the first two weeks. The sutures were removed two weeks after the procedure, and the regular oral hygiene regimen was resumed.
The gingival level of the mandibular right canine moved apically during the first two months by about 1-2 mm as compared to the level just after surgery, particularly on the mesial side. Seventy-eight percentage of the defect was covered (Table 1), and the probing depth was within 3 mm in the 6-month follow-up (Fig. 2F). The incomplete defect coverage was caused by the low interproximal bone level. The patient was satisfied with the outcome of root coverage, and the hypersensitivity symptom was improved.
Case 2
History
A 46-year-old female patient presented with generalized buccal gingival recession with hypersensitivity from the exposed roots. She was also concerned about the esthetics of the mandibular right central incisor, which had minimal buccal keratinized gingiva and an advanced gingival recession defect (Miller class III) (Fig. 3A). The mandibular right central incisor also showed interproximal bone loss radiographically (Fig. 3B).
Treatment and outcome
The procedure was similar to that in case 1. A split thickness flap was elevated at the mesial site of the mandibular right central incisor to preserve the integrity of the distal interproximal papillae. The SCTG (dimensions: 20 mm×10 mm×1.5 mm) was placed underneath the partially elevated gingiva and the exposed root surface. Distally, the flap was rotated to cover the tissue graft and sutured (Fig. 3C). The postoperative instructions were the same as those of the first patient in case 1. The gingival recession defect had 58% defect coverage, and the probing depths of all sites were within 3 mm in the 3-month follow-up (Fig. 3D) (Table 1); long-term follow-up was scheduled.
Case 3
History
A 40-year-old male complained of unacceptable esthetics of the mandibular right canine. The probing depth of this canine was within 3 mm, and mild interproximal alveolar bone loss was found on the radiographs (Fig. 4A, B) and upon clinical sounding. One-millimeter buccal keratinized gingiva was present at the mandibular right canine, and the recession was diagnosed as Miller class III (Fig. 4C).
Treatment and outcome
The procedure was similar to that of case 1. Flap flexibility was assessed (Fig. 4D), and the tissue graft (dimensions: 15 mm×7 mm×1.5 mm) was sutured to the alveolar periosteum of the mandibular right canine (Fig. 4E). The flap was rotated mesially and stabilized 1 mm above the CEJ level and 3 mm above the interproximal bone level (Fig. 4F). The gingival recession defect of the mandibular right canine had 94% root coverage in the 6-month follow-up (Fig. 4G), and the gingival level was still stable after 3 years (Fig. 4H) (Table 1).
DISCUSSION
A review published in 1996 [2] demonstrated a mean root coverage rate of 63% of the rotational flap, including 15 studies utilizing LPF and 2 studies utilizing a double papilla flap (DPF), which is a modification of LPF. These results provoked many clinicians to question the predictability of the LPF technique at that time. Conversely, from the results of studies published after 1996, LPF had a mean root coverage rate ranging from 74% to 96% (Table 2), which is comparable to the root coverage rate of CAF or CAF+SCTG [4]. Regarding the technique of LPF combined with SCTG, some articles have reported the clinical outcomes of several cases [7,18]. In Nelson [7], DPF combined with SCTG was utilized to treat the defect of a single tooth, and LPF combined with SCTG was utilized to treat multiple defects. The results demonstrated successful clinical outcomes even in advanced recession cases (88% average root coverage rate in cases with 7- to 10-mm-long defects) during a 6- to 42-month follow-up. Ricci et al. [18] utilized the same technique as Nelson [7]. The procedure had root coverage rates for treating Miller class I or II cases similar to those of the guided tissue regeneration technique at the 1-year follow-up (80.88% vs. 77.08%; the mean initial defect was 4.88 mm or 5.88 mm, respectively).
The root coverage rates in the present study, utilizing mLPF combined with SCTG, were approximately 60%-95% and were in agreement with the results of previous studies. Additionally, the cases selected in the present report are the Miller class III cases with significant interproximal bone loss (case 1) or deep, wide defects (cases 2 and 3). The involved teeth also had a limited amount of keratinized gingiva, thus causing difficulty in coronally repositioning the flap to fully cover the tissue graft. Although it has been documented that the tissue graft can be left exposed in certain situations [19], there still remain the clinical risks of having an uneven gingival margin [20]. Further, leaving a significant area of connective tissue graft exposed on the avascularized root surface may increase the chance of partial necrosis where the graft cannot receive a sufficient blood supply [21]. Thus, LPF appeared to be a superior option to CAF in these advanced gingival recession cases. LPF can ensure that the SCTG is covered by a gingival flap, which provides a sufficient blood supply laterally to increase the plasmatic circulation during initial healing [22].
In all three cases discussed in this report, the SCTG was placed about 2-3 mm above the interproximal bone level based on the concept of biological width around the periodontium, instead of solely following the CEJ level, which is the expected level of the complete root coverage, because complete root coverage is not generally expected in Miller class III cases. A retrospective study demonstrated that the complete root coverage of Miller class III recession could only be achieved in sites under certain conditions, including complete integrity of the interproximal gingiva, graft thickness greater than 2 mm, interproximal bone loss not exceeding 3 mm, and an initial recession defect width not greater than 3 mm [23]. However, our reported cases did not fulfill these requirements.
Additionally, case 3, in which the interproximal bone loss was less than that in cases 1 and 2, demonstrated the greatest root coverage rate among these cases (Table 1), indicating that the level of interproximal bone is associated with the extent of root coverage in the Miller class III cases. To elucidate the exact association between the interproximal bone level and the success of root coverage, further well-designed clinical studies are needed.
mLPF combined with SCTG placement could be a promising technique for treating Miller class III cases with significant interproximal bone loss and wide and deep recession defects. Future controlled studies are needed to provide more clinical evidence.





 XML Download
XML Download