

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Leukemia is a type of cancer that affects the bone marrow and peripheral blood, and is caused by a malignant proliferation of white blood cell (WBC) precursors. In the leukemic state, WBC-forming cells, including myeloid and/or lymphoid cells, exhibit hyperplastic changes and produce immature or abnormal WBCs, which leads to the deterioration of normal hematopoietic function. Leukemia is clinically divided into acute and chronic forms, and acute leukemia can be fatal within a few days if not appropriately treated [1]. Leukemia is further divided into lymphocytic and myelocytic forms based on histogenecity. Acute lymphoid leukemia (ALL) is more common in children, representing 50% of all neoplasms and 80% of all leukemias in childhood [2]. The prognosis of ALL is poor when it occurs in patients older than 30 years [2]. Unlike that of ALL, the incidence of acute myeloid leukemia (AML) increases with age, particularly among people older than 65 years of age, and the incidence of AML has increased significantly over the past decade [3]. The incidence of leukemia in South Korea in 2011 was 5.7 per 100,000 persons [4].
AML has been divided into subtypes M0-M7 according to the French-American-British (FAB) classification proposed in 1976, which is based on cytomorphology and cytochemistry [5]. However, the FAB classification is limited by the morphologic and genetic findings sometimes being incompatible, and the prognosis being more dependent on genetic findings than on morphologic characteristics [6]. To overcome these shortcomings, a World Health Organization classification was proposed that focuses on the genetic properties of the various leukemia subtypes: AML with recurrent cytogenetic translocations, AML with myelodysplasia-related features, therapy-related AML and myelodysplastic syndromes, and AML not otherwise specified [7].
The symptoms of leukemia are associated with the effects of neoplastic proliferation and its influence on nonneoplastic hematopoietic cells. By reducing the production of normal erythroblasts, anemia, weakness, constant fatigue, and pallor may occur. Reduction of granulocyte production may cause fever and infection. A decreased platelet level may result in spontaneous bleeding, petechiae, ecchymoses, and bruising. In addition, leukemic cells can directly infiltrate the spleen, lymph nodes, central nervous system, and gingiva.
Acute leukemia is often accompanied by oral symptoms, which are reported to be early manifestations of acute leukemia in some patients [8,9,10,11]. Oral complications such as gingival enlargement are more frequent in AML than in other types of leukemia, and it is reported that gingival enlargement occurs more frequently in the M4 and M5 subtypes [11,12,13,14]. Temporomandibular joint arthritis is usually found in AML [15], and osteolytic lesions in the mandible have been reported [16]. It may be rare to encounter leukemic patients who have oral symptoms as an early indicator of leukemia in a routine dental practice. Therefore, dentists may miss the correct timing for referral to a hematologist, which can be fatal. Stafford et al. [17]. reported that dentists are responsible for early diagnosis in a large portion of acute nonlymphocytic leukemias.
This report describes two patients who presented with gingival enlargement as an early sign of acute leukemia. We also provide a brief review of previous reports in order to highlight the required knowledge and appropriate response of dentists in this clinical situation.
CASE DESCRIPTION
Case 1
A 59-year-old female patient was referred from a local dental clinic with a chief complaint of excessive gingival enlargement that had abruptly appeared 20 days previously. The patient had hypertension but was not on any medications associated with gingival enlargement. The patient also reported experiencing a severe cold 30 days previously.
An examination revealed that the patient had generalized gingival enlargement that was more prominent in the maxilla and anterior regions. In the maxillary anterior area, there was a discrete, bulbous enlargement in the interproximal region. In the maxillary posterior area, there was diffuse enlargement, which extended to the alveolar mucosa (Fig. 1A). Gingival enlargement was most severe in the palatal area, extending beyond the cingulum of the maxillary anterior teeth (Fig. 2). The gingiva was pale blue and had a glazed texture with loss of stippling. The gingival consistency was generally friable. There was spontaneous bleeding in the canine and premolar regions of the palate.
A radiographic examination revealed generalized horizontal bone loss that was most prominent in the anterior maxillary region (Fig. 3). However, the clinical findings were more striking than the radiographic situation. Extraorally, the patient had a bruise adjacent to the right lower lip; the patient did not recall any specific traumatic injury. There was also mild enlargement and tenderness of the right cervical lymph nodes. Most importantly, the patient reported ongoing general weakness and headache. The patient's oral symptoms were suspected to be a manifestation of underlying systemic disease, and a complete blood count (CBC) with differential analysis was performed. The test results revealed a markedly elevated WBC count (71.52×103/µL), and decreased red blood cell (2.14×106/µL) and platelet (83×103/µL) counts. Immature blood cells, which are normally seen only in the bone marrow, were detected in the peripheral blood. On the basis of the clinical and laboratory findings, the patient was suspected to have acute leukemia and was referred to the Department of Hematology.
The patient was hospitalized, and further examinations were performed for a definitive diagnosis. A peripheral blood smear revealed normocytic normochromic anemia and a markedly increased WBC count (blast cells, 72%; segmental neutrophils, 18%; lymphocytes, 7%; and monocytes, 1%). Bone marrow aspiration and biopsy revealed hypercellularity (50%-60%) and an increased number of blasts, most of which were monoblasts and promonocytes. On the basis of these laboratory findings, this patient was diagnosed with acute myelomonocytic leukemia (FAB classification: AML M4).
When the definitive diagnosis had been made, dental treatment was limited to patient education regarding oral hygiene care and mouth gargling with chlorhexidine (Hexamedine, Bukwang Pharm., Seoul, Korea). Gingival enlargement was mostly resolved after the first phase of chemotherapy without any periodontal interventions. Gingival recession and dental calculus were noted in general (Fig. 4). The cervical and proximal areas of the patient's teeth were stained due to the prolonged use of chlorhexidine (Fig. 5). During the chemotherapeutic period, the patient used chlorhexidine and a soft brush continuously to prevent oral infection and inflammation. After a few cycles of chemotherapy, the patient recovered completely. Presently, the patient visits the Department of Hematology as an outpatient. No sign of recurrence has been found thus far.
Case 2
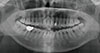
A 49-year-old female was referred for submandibular swelling, which occurred after the extraction of mandibular upper second and third molars, and generalized gingival swelling. The patient had no specific medical history. The dentist at a local clinic had extracted the teeth 2 weeks previously, and the patient developed submandibular space swelling 1 week later. The patient seemed to be indifferent to her dental status and poor oral hygiene. An intraoral examination revealed a probing pocket depth of more than 6-9 mm at all sites, easy bleeding on probing, and the presence of heavy subgingival calculus (detected on air blowing). The patient had no experience of scaling. Pus discharge was also observed in some areas. The gingival enlargement appeared like a periodontal abscess, but it was generalized. The enlargement was most severe on the lower dentition, particularly the lower left molar region, and was overly bulbous in some interproximal areas. The enlargement appeared fibrotic and friable in nature. An extraoral examination revealed swelling at the mandibular inferior border and tenderness to palpation. Routine panoramic x-ray and computed tomography also revealed severe periodontal destruction, which was considered to be consistent with the clinical findings (Fig. 6). The patient did not complain of general weakness or fever.
This patient was initially diagnosed with generalized chronic severe periodontitis, multiple periodontal abscesses, and associated submandibular-space abscess. The patient was referred to the Department of Oral and Maxillofacial Surgery, and an oral surgeon prescribed Flasinyl (metronidazole, CJ Healthcare, Seoul, Korea) and Augmentin (amoxicillin and clavulanate potassium, Ilsung, Seoul, Korea) to alleviate the space abscess. The gingival enlargement had subsided to some extent at her following visit. Accordingly, another extraction of hopeless teeth was performed to remove a possible infection source. The patient reported abrupt-onset general weakness 1 day after the extraction and visited an emergency room. The patient was hospitalized for systemic examinations. A CBC was performed, revealing a WBC count of 38.01×103/µL and decreased red blood cell (1.46×106/µL) and platelet (20×103/µL) counts. A bone marrow biopsy and genetic examination were conducted to confirm the type of acute leukemia present, and the patient was finally diagnosed with acute myelomonocytic leukemia (FAB classification: AML M4). The potential benefit of periodontal treatment and extraction to remove the possibility of oral infection during the chemotherapeutic period was explained to the patient and her family, but the patient refused the treatment. The patient submitted to a few cycles of chemotherapy and autologous bone marrow transplantation, and is in full remission. Presently, the patient visits the Department of Hematology for regular check-ups, and as yet, there has been no sign of recurrence.
DISCUSSION
Gingival enlargement can have various causes. For example, acute or chronic infection may cause enlargement involving mainly the marginal and interproximal gingiva. Specific medications such as calcium channel blockers, phenytoin, and cyclosporine are associated with gingival enlargement. More importantly, gingival enlargement may be an early manifestation of underlying systemic disease, such as acute leukemia, as in the cases reported herein.
The two patients discussed in this report exhibited severe gingival enlargement as an early sign of systemic disease, and both were diagnosed with acute myelomonocytic leukemia and received hematologic treatment. However, the diagnostic pathway should have been more sophisticated in the second case. The dentist was confused by the observation of severe bone destruction on radiography, local factors, and abscesses. The highly advanced periodontal destruction was considered to be correlated with the gingival enlargement, and therefore, the initial treatment focused on the removal of infection sources. Consequently, the patient's leukemic state was found only after subsequently expressing general weakness. The second case suggests that periodontal inflammation could be a factor that aggravates gingival enlargement associated with acute leukemia. At the sites of inflammation, leukocytes are normally trapped and recruited, and this may intensify leukemic infiltration in the leukemic state.
Leukemic gingival enlargement may be misdiagnosed because it is rarely seen in everyday dental practice; no other outpatients in the authors' department have reported gingival enlargement as an early sign of acute leukemia, as with these two patients, in more than 10 years. Moreover, most of the published studies on leukemia in the dental field have been case reports, which indicates that it is not a common situation.
Leukemia can be tentatively diagnosed by an examination of CBC. In the first case, the CBC results raised the suspicion of acute leukemia. However, the symptomatic history of a patient can play an important role in dental practice. About half of the acute leukemia patients develop symptoms such as fatigue, weakness, and feelings of helplessness within 3 months before disease onset [3]. Loss of appetite and decreased weight are also common symptoms. Fever is the presenting symptom in 10% of the patients irrespective of infection, and spontaneous bleeding and a tendency toward easy bruising are present in 5%. The two patients discussed in this report presented with systemic changes, which were crucial diagnostic clues.
If acute leukemia is left untreated or misdiagnosed, life-threatening conditions including gastrointestinal bleeding, pulmonary hemorrhage, and severe infection would develop; a majority of untreated patients might face a fatal situation within one year [18]. It is therefore very important to scrutinize the possible underlying cause of gingival enlargement in some patients, since early detection allows prompt intervention and increases the probability of survival.
Oral and periodontal symptoms are reportedly manifested in various kinds of leukemia and particularly in acute or subacute forms [19,20]. Gingival enlargement is also likely to develop in acute leukemia and in the subleukemic phase [21,22]. Moreover, specific types of leukemia (i.e., acute myelomonocytic leukemia [FAB classification: M4] and acute monocytic leukemia [FAB classification: M5] are reportedly susceptible to the gingival infiltration of leukemic cells [12,14]). Dreizen et al. [23] reported that among 1,076 adult leukemia patients, gingival hyperplasia was observed in 66.7% of those with M5, 18.5% of those with M4, and 3.7% of those with M1 and M2 leukemia. It has also been reported that gingival enlargement does not generally develop in edentulous patients [20,23], although gingival infiltration of leukemic cells was observed on fine-needle aspiration cytology in an edentulous patient with acute M4 leukemia [21].
Gingival enlargement in leukemic patients is known to disappear without any specific periodontal treatment [22]. However, enlarged gingiva facilitates plaque accumulation and food impaction, and complicates oral hygiene practice. This may lead to gingival inflammation with secondary gingival swelling. Patients in these cases are also concerned about bleeding during routine oral hygiene practice. There has been a report of a possible association between patient-reported gingival bleeding and a reduced platelet count [24]. Although plummeting platelet counts may evoke a tendency toward bleeding, Angst et al. [25] recently demonstrated that there was no statistically significant correlation between platelet count and the gingival index and bleeding on probing, and that the gingival index is, rather, related to plaque accumulation. For the patients discussed in the present report, the use of a soft brush with gentle motion and supplemental mouth rinsing were recommended.
Dentists may face a dilemma regarding whether any dental treatment will aggravate the leukemic situation and alter the patient's systemic condition [26]. Some may be concerned that while routine dental treatment and even self-performed oral hygiene practice will increase the risk of bacteremia, untreated inflammation may contribute to morbidity. The following brief guidelines may be of assistance in this context. First, patients with hematologic malignancies including leukemia should be clinically and radiologically examined for the presence of oral manifestations of the malignancies, periodontal disease, and osteolytic lesions [27,28]. Second, strict oral hygiene instructions and the removal of potential sources of oral infection should precede any cancer treatment [29]. Clinicians may frequently encounter periodontal diseases of varying degrees, and chronic periodontitis can be aggravated without specific clinical signs [26]. Therefore, scaling, subgingival debridement, mouth rinsing, extraction of nonsalvageable teeth, and administration of antibiotics should be performed prior to cancer therapy. However, all procedures should be supervised by hematologic professionals, and blood testing for preoperative evaluation is mandatory [27]. Moreover, patients in a severe or recurrent state should only be administered palliative or emergency treatment.
Gingival enlargement can be caused by underlying systemic diseases that may sometimes be lethal. The present case report describes two patients presenting with gingival enlargement as an early sign of AML. Dentists may be misguided by the rarity of this type of encounter, ignorance, or the presence of a combined infectious state, leading them to make incorrect treatment decisions. It must always be considered that oral signs and symptoms can be signs of a systemic condition.





 XML Download
XML Download