

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periodontitis is an infectious disease caused by periodontal pathogens in plaque biofilm. It is widely known that specific gram-negative bacteria play an important role in the progression of periodontitis [1]. Treatment of periodontitis is aimed at decreasing the bacterial load by removing plaque and calculus. The most effective treatment is mechanical debridement by nonsurgical methods such as scaling and root planing (SRP). However, SRP may fail to completely eradicate subgingival pathogens in unreachable areas such as deep pockets, root concavities, and furcations. Antimicrobial therapy combined with SRP may suppress these pathogens, but systemic antimicrobial agents have potential side effects such as gastrointestinal disturbance and allergic reactions. Moreover, their frequent and inappropriate use can cause bacterial resistance [2]. From a periodontal viewpoint, the major drawback of systemic antibiotics is that their concentration in the gingival crevicular fluid is insufficient to suppress the periodontal pathogens in subgingival biofilm [3].
To overcome these limitations, antimicrobial photodynamic therapy has been suggested as an adjunct or an alternative method to conventional treatment modalities. It is based on light-induced inactivation of bacteria and has two essential components: a photosensitizing agent (e.g., toluidine blue O and methylene blue) and light energy. The photosensitizer binds to the outer membrane of the target bacteria, is activated at a specific wavelength of light [4], and releases singlet oxygen and free radicals, which are extremely toxic to the mitochondria and nucleus of microorganisms [4]. Photodynamic therapy was originally developed to target tumor cells and has been used for treating cancer [5]. In the field of dentistry, several studies have shown that photodynamic therapy along with a photosensitizer can destroy periodontopathogenic bacteria in a biofilm [6,7,8]. Other experiments using methylene blue or toluidine blue O, however, have indicated that oral pathogens are resistant to this modality and are incompletely eradicated [9,10]. Many studies have been conducted using a photosensitizer and have reported controversial findings on the clinical and microbiological benefits in comparison with the traditional periodontal therapy. Clinical trials to evaluate the effects of photodynamic therapy in the management of periodontitis have been performed as an adjunct with or without SRP. A randomized clinical trial by Balata et al. [11] did not suggest any definitive benefits for photodynamic therapy along with SRP in the treatment of severe chronic periodontitis. Other studies including clinical trials by Andersen et al. [12] and Betsy et al. [13] have shown significant improvement when photodynamic therapy and SRP were performed in combination in patients with advanced periodontal disease. All of these clinical studies have utilized photosensitizers, which were applied subgingivally or topically to sites, and light sources, which were used to irradiate the sites at least once.
Recently, several studies demonstrated satisfactory results using photodynamic therapy in the absence of a photosensitizer (phototherapy, PT) in laboratory research [14] and experimental periodontitis in rats [15]. It may naturally be effective against some microorganisms associated with periodontal disease, including oral black-pigmented bacteria such as Porphyromonas gingivalis, Prevotella intermedia, and Prevotella nigrescens [4,16]. Visible light in the range of 380 to 520 nm has been shown to inactivate P. gingivalis and P. intermedia in human dental plaque samples [17]. This effect is possible because visible light activates an endogenous photosensitizer (porphyrin) in black-pigmented bacterial species and suppresses the pathogens. However, the effectiveness of continuous PT in humans has not been addressed in the literature.
The aim of this study was to elucidate the clinical and antimicrobial effects of daily PT as an adjunct to SRP in patients with chronic periodontitis.
MATERIALS AND METHODS
Participants
This single-blinded, examiner-masked, randomized controlled trial was conducted between December 2013 and May 2014 at Ewha Womans University Mokdong Hospital, Seoul, Korea. The study protocol adhered to the Declaration of Helsinki and was approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (No. 13-44A-02).
Forty-one patients with mild-to-moderate chronic periodontitis were enrolled after the study purpose was explained, and their written consent was obtained. The inclusion criteria were age of 20 years or older, presence of at least 20 teeth, and presence of at least 1 tooth with a probing pocket depth (PPD) of 4 mm or more in each quadrant. Patients with systemic diseases that could influence the outcomes, uncontrolled diabetes mellitus, pregnancy, smoking, periodontal treatment within the last six months, and systemic antibiotic therapy within the last three months were excluded. The participants were randomly divided, by coin toss, into two therapeutic groups: SRP+PT (n=21) and SRP (n=20) groups.
Treatments
Before randomization, all the participants underwent full-mouth SRP with periodontal curettes and an ultrasonic device. The SRP+PT group received electric toothbrushes with embedded light-emitting diodes (LEDs) (iBrush Inc., San Jose, CA, USA). The LEDs irradiated (single frequency, 635-nm wavelength, and 13-mW/cm2 power density) simultaneously with the vibration of the toothbrushes. The SRP group used similar electric toothbrushes without LEDs. The manufacturer's recommended irradiation time was 3 minutes per session. The patients were instructed on how to use the electric toothbrushes by verbal explanation and demonstration. All patients agreed to comply appropriately with the home care and fully adhered to our treatment instructions.
Clinical examination
The following clinical parameters were assessed before (baseline) and four weeks after (follow-up) the treatment: plaque index (PI) [18], gingival index (GI) [19], PPD, clinical attachment level (CAL), and bleeding on probing (BOP) [20]. The measurements were recorded by the same periodontist blinded to the groups at the maxillary right first molar, maxillary left central incisor, maxillary left first premolar, mandibular left first molar, mandibular right central incisor, and mandibular right first premolar. The PI and GI were expressed as scores of 0 to 3. PPD and CAL were recorded as the distances from the bottom of the pocket to the gingival margin and the cementoenamel junction, respectively, at the mesiofacial, midfacial, distofacial, distolingual, midlingual, and mesiolingual sites of every tooth. If the cementoenamel junction was not visible, a restoration margin was used. BOP was recorded as present or absent within 30 seconds of probing at the six sites per tooth.
Microbiological examination
Subgingival plaque samples were collected from the deepest pockets of each quadrant at the baseline and follow-up points by the same periodontist. In brief, the supragingival biofilm was removed by using sterile cotton pellets; each site was dried and isolated from the saliva with sterile cotton rolls; and a sterile periodontal curette was inserted into the periodontal pocket to collect the subgingival biofilm. The four samples from each participant were immediately suspended in 1.5 mL of sterile distilled water and stored at -20℃. They were then sent to a laboratory and analyzed by real-time polymerase chain reaction to identify the following microorganisms: Aggregatibacter actinomycetemcomitans, P. gingivalis, Tannerella forsythia, Treponema denticola, P. intermedia, Fusobacterium nucleatum, Parvimonas micra, Campylobacter rectus, Eikenella corrodens, Streptococcus mutans, and Streptococcus sobrinus. Bacterial amounts were expressed as genome equivalents and log-transformed.
Sample size calculation
The sample size was calculated to provide 80% power to recognize a significant difference of 1 mm in each group regarding PPD, with a standard deviation of 0.8 and 95% confidence interval. Accordingly, a sample of 18 subjects per group was required. Considering a possible dropout rate of 15% during the study period, the sample size of 21 subjects in each group (42 in total) was calculated.
Statistical analysis
Data were analyzed by using commercial IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). P-value for differences between groups using the Student t-test (age and BOP) and chi-square test (gender, smoking, and diabetes mellitus). They were assessed for normality by using the Kolmogorov-Smirnov test. As three clinical parameters (PPD, CAL, and BOP) followed normal distribution, parametric methods were used for analyzing data. To evaluate the PI and GI, Fisher exact test and McNemar test were used for the categorical variables. Student t-test was used for finding a significant difference from the baseline to the follow-up within the test and the control groups. Microbiological data were also analyzed by Student t-test. The level of significance was set at a=0.05.
RESULTS
Clinical outcomes
Forty-one participants were enrolled in this study. Three patients dropped out during the study period, so 38 patients completed the study (Fig. 1). Their mean age was 36.28±10.25 years (23-58 years). None reported any complication related to PT, such as burns, ulceration, or pain. The groups were balanced in terms of gender, smoking status, and clinical parameters at the baseline, except for age (Table 1).
The SRP+PT and SRP groups showed baseline PPDs of 2.80±0.40 and 2.76±0.52 mm, respectively. At the follow-up assessment, the clinical values decreased. In particular, PPD showed a significant reduction in the SRP+PT group (P<0.05) (Table 2). No statistically significant differences in PI and GI were observed between the groups at four weeks after the treatment (P>0.05) (Table 3). Furthermore, PPD and CAL changed significantly in the SRP+PT group compared with the SRP group (P<0.05) (Table 4). At four weeks posttreatment, all patients showed a significant decrease in PI from the baseline (P<0.05) (Table 5). BOP did not show significant changes in either of the groups.
Microbiological outcomes
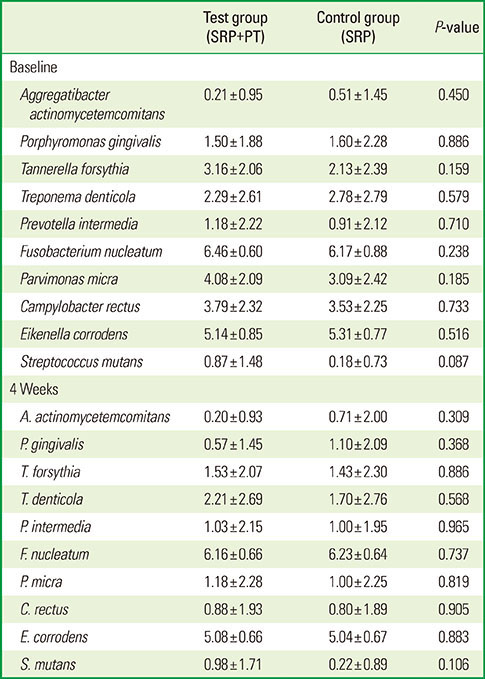
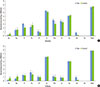
The total amounts of tested bacteria were similar in the groups (Table 6 and Fig. 2). P. gingivalis levels decreased after both the treatments. T. forsythia showed a slightly greater change in the SRP+PT group than in the SRP group, but this difference failed to reach a significant level. Bacterial DNA quantities in the subgingival biofilm did not reveal significant reductions four weeks after SRP and PT.
DISCUSSION
The present study was designed to evaluate the effectiveness of adjunctive PT by using an electric toothbrush with an embedded LED for treating chronic periodontitis. To the best of our knowledge, this is the first randomized controlled trial of daily PT in human periodontitis. Similar randomized controlled trials of photodynamic therapy have recently been published, but most utilized photosensitizers [6,7,11,12,13].
The patients performed PT thrice daily for a month by themselves, at home, after conventional mechanical debridement. Both therapeutic modalities (SRP+PT and SRP alone) led to clinical improvements. BOP was observed in more than 80% of the patients in both the groups at the baseline, but it fell to 49% and 52% in the SRP+PT and SRP groups, respectively. Likewise, PI, GI, and CAL significantly improved from the baseline values, significant differences were not found between the groups. The improvements could be attributed to the effects of mechanical debridement and/or electric toothbrushing. PPD was significantly different between the groups at the follow-up assessment: 2.04±0.42 mm in the SRP+PT group versus 2.41±0.22 mm in the SRP group. Nevertheless, almost 50% of the patients had persistent BOP after PT. This result implies that gingival inflammation did not improve despite the significant reduction in PPD.
Changes in PPD and CAL were greater in the SRP+PT group, supporting some clinical and experimental findings of the beneficial effects of PT as an adjunct to SRP. Experimentally induced periodontitis transiently reduced after photodynamic therapy in rats [15]. Likewise, diabetic rats showed resolution of periodontitis after photodynamic therapy using a photosensitizer (toluidine blue) [21]. However, several human studies revealed conflicting results [6,13,22,23,24]. Betsy et al. [13] demonstrated that the use of the photosensitizer after SRP significantly reduced PPD and CAL at 3 and 6 months after the treatment compared with SRP alone. In contrast, in a recent split-mouth randomized trial, a single application of photodynamic therapy after SRP did not provide additional benefits in clinical parameters or inflammatory markers compared with SRP alone [25]. Bassir et al. [26] also reported that two cycles of irradiation of photodynamic therapy did not result in clinical improvement in patients with moderate-to-severe periodontitis. The discrepancy could be explained by the insufficient irradiation time. Further, in a majority of the conflicting studies, photodynamic therapy was performed by the application of a photosensitizer in the periodontal pocket and exposure to visible light via a fiber-optic probe. When photodynamic therapy was performed, an antimicrobial photosensitizer was a prerequisite to bind to the target bacterial cells and was activated by light of a specific wavelength. Various photosensitizers currently available for use in clinical studies are as follows: porphyrins [27,28], chlorins [29,30], phthalocyanines [31,32], and phenothiazines [6,13,23,25,26]. Phenothiazines (toluidine blue O and methylene blue) were most frequently used as photosensitizers in the field of dentistry and thought to lead to better clinical results. However, despite the photosensitizer's absence, our clinical results revealed that daily LED irradiation provides significant improvements in terms of PPD and CAL. These observations suggested that the clinical advantages of adjunctive PT could be accomplished even in a photosensitizer-free environment. Endogenous porphyrins of black-pigmented anaerobes such as P. gingivalis, P. intermedia, and P. nigrescens might act as the potential photosensitizer and are thought to be involved in the inactivation of microorganisms [33].
Subgingival bacterial recolonization occurs immediately after SRP. Ongoing periodontal therapy is crucial for maintaining appropriate levels of periodontal pathogens. Several in vitro studies have shown the bactericidal effect of photodynamic therapy against periodontopathogenic bacteria [8,33,34]. Daily photodynamic therapy with a high-power blue LED and red photosensitizer has growth-inhibiting effects on P. gingivalis [35]. Moreover, Komerik et al. [34] found that photodynamic therapy inactivates P. gingivalis protease, a virulence factor, and suppresses the viability of P. gingivalis. Similarly, another microbiological study indicated the growth inhibition of periodontal pathogens by 405-nm light irradiation, suggesting that visible light without a photosensitizer might suppress the growth of P. gingivalis [14]. In contrast, clinical studies have shown no antimicrobial benefits of photodynamic therapy [22,23], as noted in the present study. Although the amounts of periodontopathogenic bacteria, such as P. gingivalis and T. forsythia, in the subgingival biofilm were lower in the SRP+PT group than in the SRP group, a significant intergroup difference was not obtained.
In conclusion, adjunctive PT seems to have clinical benefits, but evidence of its antimicrobial effects is insufficient. Long-term studies are necessary to establish the most effective PT protocol (i.e., irradiation time, intensity, and distance of light source) for the treatment of periodontitis and to compare the effectiveness of PT with and without exogenous photosensitizers.






 XML Download
XML Download