

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Various augmentation procedures have been introduced to treat a resorbed alveolar ridge, including guided bone regeneration with particulate or block-type materials, distraction osteogenesis, and ridge splitting [1,2]. Four crucial factors have been proposed in obtaining successful bone augmentation beyond the envelope of skeletal bone: primary closure, angiogenesis, space creation and maintenance, and stability of the blood clot [3]. Among these factors, the ability to maintain space has been highly emphasized, especially for large defects, and hence the use of bone block grafts has been favored by clinicians due to their dimensional stability and resistance to deformation in unprotected areas that are subject to compressive forces such as mastication [4].
A large body of literature indicates that the particulate or block-type autogenous bone is the gold standard for bone augmentation [5,6]. In order to maximize the success of an onlay bone graft, several factors should be considered: the influence of perforations or decortication on the recipient bed [7,8,9], revascularization rates [10], microarchitecture of the bone graft [11], and the influence of embryonic origin [12]. In previous studies, the authors have evaluated the effect of perforation of bone blocks and decortication of the recipient bone [8,9], and observed rapid integration of an autogenous bone block (ABB) graft onto the recipient bone bed. Thereafter, the authors subsequently questioned the necessity of rigid fixation of a bone block.
A limited number of studies have investigated the role of rigid fixation and emphasized its importance [8,9,13,14]. Phillips and Rahn [13,14] showed that the amount of resorption of onlay bone grafts with rigid fixation was less than that of the grafts which were not fixed. La Trenta et al. [15] showed that endochondral bone grafts without rigid fixation healed with a predominately fibrous union. It has also been proposed that movement of the grafted materials during the early stages of wound healing could lead to failure of osseointegration by differentiation of mesenchymal cells into fibroblasts instead of osteoblasts [16]. However, recent studies have shown contradictory results [5,17]. Lin et al. [11] have reported the possibility of vertical augmentation without fixation in a rabbit model, and no difference was shown in graft volume retention or graft survival between the fixed and nonfixed conditions in a low-motion region. However, there is still controversy surrounding the results of bone block grafting without rigid fixation.
Therefore, the objectives of this study were to observe the incorporation of ABB in comparison to hydroxyapatite (HA) block (HAB) without rigid fixation onto rabbit calvaria, and to compare the healing pattern over two different healing periods of 4 and 8 weeks.
MATERIALS AND METHODS
Experimental animals
A total of 16 male New Zealand white rabbits (3.0-3.5 kg; n=8 at 4 weeks, n=8 at 8 weeks) were used in this study. The animals were kept under standard laboratory conditions, fed a standard diet, and raised in separate cages. The animal selection, management, surgical protocol, and preparation followed routines approved by the Institutional Animal Care and Use Committee, Yonsei Medical Center, Seoul, Korea (certification #2010-070).
Fabrication of the HAB scaffold
A simple porous scaffold was produced according to previously published methods [18]. In brief, the sol-gel process was used to prepare the HA nanoparticles. Selected precursors of the HA sol used in this study were Ca(NO3)2-4H2O (99%; Sigma-Aldrich, St. Louis, MO, USA) and P(OCH2CH3)3 (97%; Sigma-Aldrich). The Ca precursor was dissolved in methyl alcohol at a stoichiometric Ca:P ratio of 1.67. The solution was dehydrated at 180℃ after solvent evaporation, and the solution was refluxed in methyl alcohol in an Ar atmosphere. The prehydrolysis of the P precursor was carried out over 10 hours; HCl and H2O were added as catalysts before the reaction reaction with the Ca precursor. The two precursors were reacted to prepare the HA solution, which was subsequently dried at 950℃. The prepared HA nano powder was stored at 50℃ in a drying oven.
The HA scaffold was fabricated using template casting methods. The HA slurry was made by dispersing the nano HA powders into vehicle solution. The vehicle solution was prepared using organic additives (5% polyvinyl alcohol, 1% methyl cellulose, 5% ammonium polyacrylate dispersant, and 5% N,N-dimethylformamide drying agent). The polyurethane sponges used as a template were coated with slurry and dried at room temperature for 12 hours, and the HA scaffold was sintered at 1,250℃ for 3 hours. The HA scaffold was coated again with slurry and resintered. The finished scaffold was an 8-mm diameter and 3-mm-high disk with porosity, specific surface, strut thickness, and strut spacing of 81.5%±1.5%, 31.2±1.3 mm2/mm3, 140.1±4.3 µm, and 523.1±4.4 µm, respectively, according to a previous study [19]. A hole was created in the center to provide a better blood supply to the block.
Experimental procedure
The animals were anesthetized with an intramuscular injection of a mixture of ketamine hydrochloride (Ketalar, Yuhan, Seoul, Korea) and xylazine (Rompun, Bayer Korea, Seoul, Korea). The surgical sites were shaved and then swabbed with alcohol and povidone iodine, and then a local anesthetic (2% lidocaine; lidocaine HCl, Huons, Seoul, Korea) was administered. An incision was made along the sagittal midline from the frontal bone to the occipital bone. A full-thickness flap was elevated to expose the cranial bone. Two standardized circular grooves that incompletely penetrated the skull were prepared as the recipient beds in the bone on each side of the midline using a trephine bur (diameter, 8 mm). Four cortical perforations within the circle were then drilled to induce bleeding from the marrow space with a 1.5-mm diameter carbide bur. The handpiece was operated at 800 rpm under copious irrigation using saline refrigerated at 4℃ with a flow rate of approximately 50 mL/min. Four cortical perforations within the circle were then drilled to induce bleeding from the marrow space with a 1.5-mm diameter carbide bur. ABB was obtained from the posterior rabbit calvaria using a trephine bur of the same diameter, and then the synthetic HAB and the ABB were positioned on the prepared recipient beds without fixation (Fig. 1). The soft tissues were repositioned and then sutured layer by layer with a resorbable suture material (4-0 Vicryl, Ethicon, Somerville, NJ, USA) to achieve primary closure. The stitches were removed after 10 days. The animals were sacrificed at 4 or 8 weeks postoperatively [20], and block sections of the graft sites were collected and prepared for radiographic and histomorphometric evaluation.
Histologic evaluation
The harvested block sections were fixed in 10% buffered formalin and decalcified with 5% formic acid for 14 days. Paraffin wax blocks were made and sectioned in the mesiodistal direction at a thickness of 5 µm. The sections were stained with hematoxylin and eosin. General histological findings were observed under a microscope (Olympus BX41, Olympus Co., Tokyo, Japan).
Tomographic evaluation
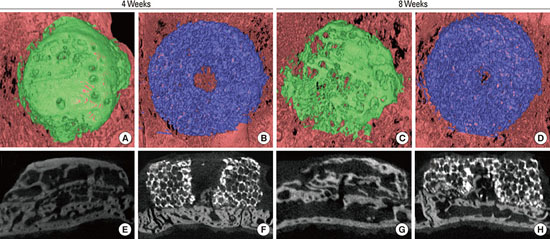
The fixed block specimens were scanned using a microcomputed tomography (micro-CT) system (SkyScans1072, SkyScan, Aartselaar, Belgium) at a resolution of 18 µm (100 kV and 100 µA). The scanned sets of data were processed in DICOM format, and OnDemand three dimensional (3D) software (Cybermed, Seoul, Korea) was used to reconstruct the area of interest (Fig. 2). The overall dimensional topography of the grafts and recipient beds was visualized with a 3D-reconstructed image, and the residual volume (in mm3) of the block graft was measured in 3D-reconstructed images.
Histomorphometric evaluation
The histologic and radiographic analysis was performed by one experienced researcher (S.Y.B.). An automated image analysis system (Image Pro Plus, Media Cybernetics, Silver Spring, MD, USA) was used for the histomorphometric analysis. The following values were measured:
(1) Augmented area (mm2): the area of all tissues beyond the cranial vault.
(2) Vertical height (mm): measured 1 mm away from the lateral and medial boundaries in the center of the augmented block.
(3) New bone (mm2; %): only the area with newly formed miner-alized bone (mm2) shown in the HAB group.
Statistical analysis
Mean and standard deviation values were calculated for each group from the measurements taken from the central section of each of the grafted materials and the 3D micro-CT data. Statistical differences were determined by two-way analysis of variance and a post hoc t-test for multiple comparisons, and by an unpaired t-test for comparisons between two independent groups using the statistical software program SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). The critical value was set at [α]=0.05.
RESULTS
Clinical findings
Surgical wound healing was uneventful throughout the experimental period. No complications were observed, including wound dehiscence, severe swelling, or bleeding.
Tomographic findings: micro-CT
A shift in the location of the integrated graft materials was clearly observed in six ABB specimens (three at 4 weeks and three at 8 weeks) and ten HAB specimens (five at 4 weeks and five at 8 weeks). For the ABB group, distinctive external resorption was observed at 4 weeks of healing, and the bone resorption was lowest at the central area and highest at the boundary area, resulting in a dome-shaped appearance; there was minimal resorption in the HAB group at this stage. External resorption became clearly evident at 8 weeks of healing at the boundary area in the grafted ABB, while there was still minimal resorption in the grafted HAB and its morphology appeared intact, maintaining its original shape. The total volumes of grafted ABB and HAB were measured using micro-CT analysis and are presented in Tables 1 and 2.
Histologic findings
ABB group
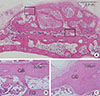
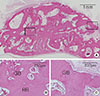
Histological integration of the graft and the recipient bed was observed in all groups at both healing periods. At 4 weeks, the graft-recipient bed interface exhibited a bony bridge connection after intense remodeling in the area adjacent to the graft; however, three of the specimens at 4 weeks and one at 8 weeks contained small areas of connective tissue partially interposed between the graft and the recipient bed. A few osteoclasts were observed along the bone block, but there was no sign of foreign body reactions or severe inflammation. The block presented an absorbed appearance at the lateral borders and the upper surface, displaying a rounded rectangular shape with an irregular border, and increased adipose tissue invaginations were observed in the intramedullary space (Fig. 3). At 8 weeks, the resorption processes appeared to have continued, resulting in a dome-shaped appearance rather than rectangular block shape. The remodeling along the interface between the recipient bed and the graft had progressed further, so it was difficult to distinguish the interface between the grafted bone and the recipient bed. The maturation of the grafted bone block appeared to have progressed further than at 4 weeks, and a large amount of adipose tissue was observed in the intramedullary space (Fig. 4). However, the overall area of adipose tissue appeared to have decreased in comparison to the area at 4 weeks.
HAB graft
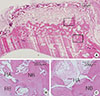
At 4 and 8 weeks, the grafted HAB materials were well maintained under the connective tissue layer, and there was little or no change in the perimeter at either point in time. There was no sign of severe inflammation or exposure of the material. Intimate contact between graft materials and the recipient bed at the interface surface-indicating bony union-was observed in both groups. The HAB appeared to be infiltrated by newly formed bone, without signs of necrosis or osteolysis, and direct contact was observed between the newly formed bone and the graft materials, especially at 8 weeks. Newly formed bone was observed along the interface between the recipient bone and the block, and extensive vascular tissue was observed within the remaining graft materials. Resorption of graft materials was barely noticeable over the healing period (Figs. 5 and 6).
Histometric analysis
The results of the histomorphometric analysis are presented in Tables 1, 2, 3. The total area of both the ABB and HAB grafts did not show any statistically significant differences between 4 and 8 weeks postoperatively (P>0.05). The presence of dislocation did not affect the results, and the height of the augmented area of the ABB and HAB grafts also did not differ significantly between ABB and HAB.
DISCUSSION
In the present study, we observed the tomographic and histological changes of synthetic HAB and ABB without rigid fixation on rabbit calvaria, and demonstrated that both grafts successfully integrated onto the recipient bed without any stabilizing methods. There was some resorption of autogenous bone, but no foreign body reaction or inflammation was observed.
The rabbit calvarial model has been used as a bone-defect model for a non-load-bearing site and for evaluating various biomaterials and regenerative techniques due to its resemblance to human mandibular bone, which has a poor blood supply and limited bone marrow [21,22]. In the present study, we evaluated the outcome of these graft materials at 4 weeks postoperatively, which represents the early phase of the healing response, and measured properties such as the stability of the materials and host reactions; at 8 weeks postoperatively, which represents the late healing response, we measured processes such as bone incorporation, resorption of materials, bone remodeling, and the amount of bone regeneration [22].
Regarding the rigid fixation of bone block grafts, numerous studies have demonstrated the need for a rigid fixation that can avoid fracture at the graft-bed interface since the mechanical stability of the grafted materials is essential to minimize micromovement during the initial healing phase. Previous studies have demonstrated that rigid fixation reduces resorption and increases the success rate of the ABB graft [13,14], while a lack of rigid fixation induces predominantly fibrous union between the endochondral ABB graft and recipient bed [15]. On the other hand, some studies have found successful graft volume retention and survival without rigid fixation [5,11]. In the present study, both the HAB and ABB without rigid fixation were successfully incorporated onto the recipient bed although the location of the graft material had clearly shifted before integration into the recipient bed in six ABB specimens (three at 4 weeks and three at 8 weeks) and ten HAB specimens (five at 4 weeks and five at 8 weeks). Generally, the rabbit calvarium is considered to be a region free of pressure and movement, but some of the typical behaviors of rabbits, such as grooming, can have an undesirable effect on graft material stability. Nevertheless, successful integration between the recipient bed and bone graft was observed at 4 and 8 weeks postoperatively in all of the groups.
Histological analysis was performed only on representative central cross-sectional views, and was not sufficient to observe 3D changes of wound healing events. Therefore, 3D micro-CT was used in this study to observe the overall healing pattern of the graft materials. Definite external bone resorption was observed in micro-CT images at 4 weeks for the ABB grafts, and continued resorption was noted at 8 weeks, although the difference in mean volume between the two points in time was not significant. Meanwhile, in the HAB graft, there was no sign of resorption and the graft appeared to remain intact.
According to our histologic analysis and 3D micro-CT evaluation, the tendency toward the progression of bone resorption in the grafted ABB material implies that the augmented ABB could be unpredictably resorbed, while the volume of the synthetic HAB graft was maintained throughout the 8-week postoperative period. The area of new bone in the HAB group tended to increase between 4 and 8 weeks, although again, the difference did not reach statistical significance. Furthermore, the total area of new bone and the remaining grafted materials in the HAB group was lower than the mineralized area of the augmented ABB at both healing periods; it nevertheless appeared sufficient to achieve complete integration. New bone had infiltrated to two-thirds of the overall height in three specimens at 4 weeks and four specimens at 8 weeks, suggesting that HAB has substantial potential in vertical bone augmentation procedures even without fixation (data not shown).
Several long-term studies have demonstrated that HA can be used in the treatment of atrophic ridges as a predictable and stable biomaterial [23,24,25]. However, the success of HA is limited primarily due to its slow degradation rate [26]. The quality and quantity of newly formed bone can only be maximized when the degradation rate is similar to the rate of bone formation [27,28]. It has generally been believed that HA is nonresorbable; however, different types of HA have different resorption rates [29,30], and the resorption rate and mechanical strength of HA can be controlled by varying its porosity, the sintering method used in its production, and the composition of the graft material itself [27,28,29,30]. In vertical bone augmentation beyond the bony envelope, as in the present study, a slow degradation rate appears advantageous, as it allows the graft material to maintain its volume and provide space. Furthermore, the authors have previously shown that an HA scaffold can be applied to tissue engineering technology by using mesenchymal stem cells or various growth factors [31,32,33]. Therefore, future studies might consider the application of growth factors or stem cells in HAB for vertical bone augmentation without fixation.
In conclusion, both ABB and synthetic HAB were successfully incorporated onto the recipient bone bed despite the lack of fixation, and appeared to maintain their volume over the healing period without any severe resorption.






 XML Download
XML Download