

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Since the dental implant was first introduced, various fixture designs and surface treatments have been developed for enhancement of osseointegration [1,2]. These designs aimed to achieve implant treatment with less time required for the healing period and longer-term clinical stability. Along the above-mentioned lines, machined-surface dental implants were replaced by those with rough surfaces [3]. Notably, sand-blasted, large-grit, acid-etched dental implants not only provide extensively increased contact area with adjacent alveolar bone tissue [4], but also enhance cell attachment for de novo bone formation onto the implant surface [5].
Dental implants are supported by underlying bone tissue via direct bone contact (osseointegration); therefore, increasing the bone-to-implant contact area has been a main research topic in implant dentistry [6,7]. In previous studies, newly formed bone could be observed on the dental implant surface even in fatty marrow areas [8], in which increased bone density was observed around the dental implant compared to the marrow area. These findings can be explained by contact osteogenesis in Davies' hypothesis [5,9]. The author described the mechanism of peri-implant bone healing, in which two types of healing are characterized: differential bone formation from recipient bone (distance) and attached cells onto the implant surface (contact osteogenesis). Therefore, cellular events, including attachment, proliferation, and differentiation on the dental implant surface have been suggested to be the most important factors for peri-implant bone healing and, additionally, Davies [5] proposed that surface topographies also affect contact osteogenesis. Many other studies have proven his hypothesis by demonstrating increased bone-implant contact around rough-surfaced implants [10,11], such as sandblasted, large-grit, and acid-etched surfaces, compared to those with machined surfaces [12,13].
According to the theory of contact osteogenesis, the microtexture of a rough surface could retain fibrin complex on the surface, and enable enhanced attachment and migration of undifferentiated cells, which are the initial steps of bone formation [9,14]. Since the clinical success of these rough surface implants [3,15], various other approaches have been developed for focusing on enhancing cellular events on the modified surfaces, that is, hydrophilic or anodized implant surfaces [16,17,18,19]. However, the separate effects of cellular events, such as cell attachment and differentiation, have not yet been elucidated.
The current development of implant surface technology has targeted the generation of a "biomimetic surface" on dental implants [1,20], in which biologic molecules have been applied onto the implant surface to stimulate osteogenesis and mimic each developmental step in the healing process. Extracellular matrix, peptides, and various growth factors are representative biologic molecules. Fibronectin is a major extracellular matrix that mediates attachment of cells to other cells or to other surfaces, such as the basement membrane. Recent studies have introduced a fibronectin-coated dental implant system in the research stage [21,22], and immobilization of fibronectin increased cell attachment [23] and osteoblastic protein expression at the in vitro level [24]. Another strategy in creating biomimetic implant surfaces is the use of growth factors [25,26] or their natural substitutes, such as oxysterol [27], for enhancement of osteogenic cell differentiation. Previous studies have demonstrated that oxysterols regulate differentiation of stem cells into osteogenic cells via the hedgehog pathway, and also prevent adipogenic differentiation in vitro [28,29]. Another in vivo study also found increased bone healing and augmentation in a spinal fusion model in animals [30].
Even though these two types of biomimetic implant surface developments showed increased cell attachment and differentiation in vitro [23,27], there was a lack of enhancement of osseointegration by using fibronectin or oxysterol in clinically-mimicking an in vivo animal model. Therefore, the present study aimed to evaluate the effects of fibronectin and oxysterol immobilized on machined-surface dental implants for the enhancement of cell attachment and osteogenic differentiation, on peri-implant bone healing in the early healing phase using an experimental model in dogs.
MATERIALS AND METHODS
Animals
Five male mongrel dogs, aged 18-24 months and weighing approximately 30 kg, were used. All of the dogs had intact dentition and a healthy periodontium. Animal selection, management, and preparation, as well as the surgical protocol, followed the routine procedure approved by the Animal Care and Use Committee, Yonsei Medical Center, Seoul, Korea (2011-0072-1).
Implant preparation
Machined-surface implant (MI)
Cylindrical, threaded implants of commercially pure titanium (Ø3.4 mm, 10-mm length) with a machined surface were provided from the Research Institute of Dentium, Seoul, Korea.
Apatite-coated MI (AMI)
The MI was treated by calcium phosphate (CaP) nano-coating at a thickness of 500 nm, using ion beam-assisted deposition, as described previously [22]. For apatite formation on CaP-coated surfaces, samples were immersed into the solution, including Dulbecco's phosphate-buffered saline (DPBS, Gibco-BRL, a division of Life Technology, Grnad Island, NY, USA) and reagent grade CaCl2 (100 mg/L). Apatite-coated samples were then rinsed with distilled water twice and dried at ambient temperature.
Fibronectin-loaded and AMI (FAMI)
FAMI samples were fabricated using the same method as for AMI, except that DPBS solution containing fibronectin was used instead of normal DPBS.
Oxysterol-loaded and AMI (OAMI)
CaP-coated, MIs were immersed in DPBS solution containing oxysterol for 2 days, and washed three times with distilled water and dried. The samples were immersed again in DPBS solution without oxysterol for one more day for additional apatite coating on the oxysterol/apatite coated surface, and then washed and dried.
Study design and surgical protocol
Ten experimental groups were allocated according to the type of implant surface (MI, AMI, FAMI, OAMI, and SLAI) and observational period (2 and 4 weeks). Five types of implants were installed in a randomly selected unilateral edentulous ridge, and the same types of implants were installed on the contralateral side at 2 weeks after the first surgery. The order of installation sites was rotated in five animals for even distribution of the experimental site. After allowing differential healing periods (2 and 4 weeks) following implant installation surgery, the animals were sacrificed for histological analysis.
Twelve weeks before implant installation surgery, all premolars and first molars were extracted at both mandibles under general anesthesia and sterile conditions in an operating room using 0.05 mg/kg atropine (subcutaneous injection), 2 mg/kg xylazine (Rompun, Bayer Korea, Seoul, Korea), and 10 mg/kg ketamine hydrochloride (Ketalar, Yuhan Co., Seoul, Korea) intravenously. The dogs were placed on a heating pad, intubated, administered 2% enflurane, and monitored with an electrocardiogram. After disinfecting the surgical sites, 2% lidocaine HCl with epinephrine 1:100,000 (Kwangmyung Pharm, Seoul, Korea) was administered by infiltration at the surgical sites. Implant installation operations were also performed under the same conditions as the tooth extraction procedure. A midcrestal incision was made, and mucoperiosteal flaps were carefully reflected on the buccal and lingual aspects. The edentulous ridge was carefully flattened with a surgical bur under sterile saline irrigation in order to obtain a widened ridge to accommodate a standardized ridge shape. Five prefabricated implants were installed in rotational order from anterior to posterior sites in individual animals with an even distribution of installed sites in each group, and the same order of installed implants was applied at both sides of the edentulous ridge in the same animal. Implant site preparation was performed by sequential drilling, and the flaps were sutured after implant installation using 5-0 resorbable suture materials (Vicryl 5/0, Polyglactin 910, Ethicon, a division of Johnson & Johnson, Somerville, NJ, USA). The sutures were removed after 7-10 days, and a soft diet was provided throughout the study period.
Histologic preparation
The animals were sacrificed with an anesthesia drug overdose, and block sections, including segments of implants, were preserved and fixed in 10% neutral-buffered formalin. The specimens were dehydrated in ethanol, embedded in methacrylate, and sectioned in the mesio-distal plane using a diamond saw (Exakt, Apparatebau, Norderstedt, Germany). From each implant site, a central section was taken to a final thickness of about 30 µm, and the sections were stained with hematoxylin and eosin.
Histologic and histometric analysis
Histologic and histometric analyses were performed using incandescent and polarized light microscopy (Olympus Research System Microscope BX51, Olympus Co., Tokyo, Japan) and a PC-based image analysis system (Image-Pro Plus, Media Cybernetic, Silver Spring, MD, USA). The bone-to-implant contact proportion (BIC) and bone density in the space between two threads were measured along the whole length of the implants. The bone density was defined as the proportion of newly formed bone in the interthread space. At four sites among a total of 50 experimental samples, the implant apex area intruding into the mandibular canal was excluded in the histometric analysis, and this area did not exceed 2 mm in length in any of the four cases (Fig. 1).
Statistical analysis
Statistical analysis was performed using a commercially available software program IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). The linear mixed model was used to estimate the contributions of two fixed effects (types of surface treatment and observational periods) and a random effect (animal subject) to the histometric results of the bone-to-implant interface (BIC and bone density). Because there was no interaction between the two factors (P=0.457 for BIC and P=0.359 for bone density), the experimental groups in the same observational period and the same experimental groups with different observational periods were compared separately using repeated measures analysis of variance and a paired t-test, respectively. The level of significance was set at 5%.
RESULTS
Clinical observation
After the use of sequential drills and a countersink drill, all implants were installed at the final torque of 30-50 N·m on the day of implant installation. All sites underwent uneventful healing during the whole experimental period, with limited signs of inflammation and cover-screw exposure.
Histologic observation
All specimens, except one implant, showed direct bone contact with the implant surface (osseointegration) along the whole length of the dental implants. One site in the FAMI group showed fibrous encapsulation without any bone contact, and this was excluded in histometric analyses. Four among the 50 installed implants protruded into the mandibular canal, and no bone formation occurred in the protruding area; however, those lengths did not exceed 2 or 3 threads of the dental implant from the apex.
At the observational period of 2 weeks, about half of the dental implant surfaces directly contacted the newly formed bone. Notably, in specimens from the FAMI and SLAI groups, newly formed bone continuously lined the entire surface, while the MIs with and without the other coating methods showed a partial or limited lining of osseointegration (Figs. 1 and 2). Two types of bone trabecula could be observed: One type appeared to sprout from the recipient bone tissue (black asterisks in Fig. 2), and the other type was woven bone lining newly formed on the implant surface without any relationship with the recipient bone tissue (yellow asterisks in Fig. 2C and E). Most of FAMIs and SLAIs showed the latter type of bone tissue, suggesting contact osteogenesis in the healing processes of osseointegration.
Histometric analysis
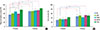
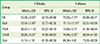
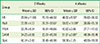
The results of histometric analyses (mean, standard deviation, and 95% confidence interval for the mean) were presented in Tables 1 and 2 and Fig. 5. Statistical analyses using a linear mixed model revealed that the BICs were significantly different between groups, according to the observational period (P<0.01) and type of surface treatment (P<0.01). At the 2-week observational period, the BIC averaged 54.08%±9.50%, 59.94%±5.49%, 68.54%±11.42%, 58.65%±8.84%, and 77.14%±7.38% for the MI, AMI, FAMI, OAMI, and SLAI groups, respectively. The SLAI group, as a positive control, showed the highest BIC among all groups, and there were significant differences from the MI (P<0.01), AMI (P=0.04), and OAMI (P=0.03) groups. Although there was no significant difference in BIC between the FAMI and SLAI groups, the FAMI group had a wider confidence interval for the mean BIC than the SLAI group; a similar maximum level of confidence interval was found in FAMI (86.70%) and SLAI (86.30%), but the corresponding values for the minimum levels of intervals were 50.37% and 67.98%, respectively. The other experimental groups (MI, AMI, and OAMI) showed a significantly increased BIC at 4 weeks compared to the same experimental group at 2 weeks (P=0.03, P=0.04, and P=0.02, respectively). In addition, there were no significant differences in BIC between any of the groups at the 4-week observational period, when the BIC averaged 70.53%±7.77%, 71.10%±11.75%, 73.95%±9.74%, 74.94%±5.55%, and 84.34%±4.06% for the MI, AMI, FAMI, OAMI, and SLAI groups, respectively.
Significantly increased bone density was found from the 2-week to 4-week observational periods in the linear mixed model (P<0.01), but no effects were found according to the type of surface treatment (P=0.134). Bone density at the 2-week observational period averaged 29.84%±11.80%, 33.99%±4.57%, 33.78%±9.34%, 34.23%±8.99%, and 42.74%±3.42% for the MI, AMI, FAMI, OAMI, and SLAI groups, respectively. The corresponding values for bone density at 4 weeks were 46.92%±9.58%, 50.82%±11.89%, 42.62%±3.96%, 51.91%±2.86%, and 50.18%±7.75%, respectively; there were significant differences from 2 weeks to 4 weeks in MI (P=0.02), AMI (P=0.03), and OAMI (P=0.01).
DISCUSSION
This study was based on our two previous studies that demonstrated an increase in cell adhesion on fibronectin and patite-coated titanium surfaces [23] and enhancement of osteoblastic differentiation by oxysterol and apatite-coated titanium surfaces [27]. Since the development of dental implants using titanium, various surface treatments have been studied to make a bioactive titanium surface through the concept of mimicking cellular events in bone formation and remodeling processes [1,20]. The two above-mentioned types of implant surfaces were also intended to transform the surface from "biotolerant" to "bioactive" titanium: The fibronectin and apatite coating was intended to promote cellular adhesion onto the surface as a first step in the healing process [23], and the oxysterol or apatite coating was intended to promote differentiation of the adhered cells [27]. However, most dental clinicians still prefer rough surface implants without any biomimetic surface modification, even though various types of biomimetic surface implants have been commercially available. A systematic review of the Cochrane Collaboration reported that there was no clinical evidence of superiority in any particular type of dental implant [31].
The present study aimed to determine whether biomimetic implant surfaces that showed greater cell attachment and differentiation at in vitro level [23,27] could enhance the histologic parameters of the bone-to-implant interface in experiments in vivo mimicking clinical situations. In the present experimental model of normal bone without any defects, two types of bone healing patterns were observed around the dental implant surface: (1) a thin rim of woven bone deposited onto the implant surface (yellow asterisks in Fig. 2); and (2) bony trabecula sprouting from recipient bone tissue and contacting the implant surface (black asterisks in Fig. 2). These correspond to distance osteogenesis and contact osteogenesis in Davies' hypothesis [5], respectively. In a previous study, Davies described contact osteogenesis, in which de novo bone formation occurred on the implant surface; this pattern of healing was also demonstrated in the present results [5,9]. At the 2-week observational period, mineralized tissue could be seen on the implant surface contacting connective tissue fibers. Furthermore, the thickness and degrees of mineralization were varied, which indicated the bone formation process originated from the implant surface rather than the recipient bone tissue.
The sites receiving FAMI showed histologic evidence of contact osteogenesis along a larger area of the implant surface compared to the other experimental groups at 2 weeks of healing. The first step in contact osteogenesis would be cell adhesion onto the implant surface, followed by further cellular events, including proliferation and differentiation [14]. Fibronectin binds to cell adhesion molecules (integrin) on the cell surface, and increases/stabilizes cell-cell/cell-stratum adhesion [32,33]; therefore, these in vivo results might be caused by the function of fibronectin, like in vitro results. This healing pattern could also be demonstrated in sites receiving SLAI as a positive control group. Numerous previous studies have already found increased bone-to-implant contact in SLA-surfaced implants compared to MIs, which resulted from increased surface energy by microroughness of the surface [13,34,35]. In the histometric results, the SLAI group showed a higher BIC compared to the other three experimental groups (MI, AMI, and OAMI), and there was no significant difference between the FAMI and SLAI groups. However, the FAMI group also did not show any differences from the other groups, unlike the SLAI group. While the SLAI group showed a narrow range of histometric results, sites receiving FAMI showed a relatively wide range of results with regard to the BIC proportion; 95% confidence intervals for the mean were 67.98-86.30 in the SLAI group and 50.37-86.70 in the FAMI group. Rough surface implants can provide increased contact surface and mechanical interlocking with the recipient bone tissue [11,36], and these might increase the stability of SLAI during the early healing period. Increasing the stability of implants could also stabilize the in vivo healing process, which can be influenced by not only cellular events, but also the various environments of the recipient site (bone quality, biologic responses by cytokines, and immune responses). For this reason, FAMI might show a less uniform increase in the BIC compared to the SLAI, despite enhancement of cell adhesion.
Oxysterol is an oxidized derivative of cholesterol, and its novel characteristic of regulating differentiation into osteogenic cells has been the subject of increasing research attention. In previous studies, oxysterol induced in vivo osteogenesis like bone morphogenetic protein-2 (BMP-2), or synergistically increased the osteoinductive effects of BMP-2 [30,37,38]. Since complications of BMP-2 application have emerged in research and clinical fields [39,40], oxysterol has received attention as a substitute or regulating factor for BMP-2. Our previous study also showed an increase in alkaline phosphatase with oxysterol surface coating, and simultaneous apatite and oxysterol coating could synergistically enhance in vitro osteogenesis [27]. In the present study, the authors hypothesized that osteoinduction by oxysterol could enhance bone formation by osteoblasts adhered to the implant surface, and increase the BIC and bone density in the early healing phase. However, oxysterol coating on the implant surface failed to enhance the BIC and bone density in the space between threads, and these findings are in agreement with a previous study [26] that demonstrated that implant surface coating with recombinant human BMP-2 did not increase the BIC or bone density in a nondefect, normal bone area, despite successful vertical augmentation in the supra-alveolar defect area without any graft materials [25,26]. Osteoinductive molecules might not accelerate or enhance bone healing at the bone-to-implant interface in normal bone, even though they can increase bone formation in the area with unfavorable defects. However, to confirm these hypotheses, further studies should be performed in various defect models.
This study aimed to determine the effects of enhancement of cell adhesion onto the implant surface and osteogenic differentiation by surface coating techniques on bone healing processes, especially at the bone-to-implant interface, in the early healing phase. Two types of implants focusing on cell adhesion increased the BIC at 2 weeks after implant installation: sand-blasted/acid-etched and fibronectin-coated surface implants. However, surface coating with osteoinductive molecules did not modify the BIC or bone density around any of the implant surfaces. Cell adhesion onto the implant surface may enhance contact osteogenesis around the implant in the early healing phase, when the implant is installed in normal bone without any defect.




 XML Download
XML Download