

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periodontitis is an inflammatory disease of the dental apparatus caused by specific microorganisms with clinical manifestations of periodontal ligament and alveolar bone defects. Periodontitis is one of the most common infective diseases in the world that can lead to tooth loss. Thus, early detection and treatment of this disease is important [1,2,3]. Evaluation of bone levels by radiography is one of the best paraclinical methods in the diagnosis of periodontitis. Sometimes it is impossible to detect periodontal disease or evaluate the prognosis of the teeth without a good radiograph [4,5]. There are some technical errors in radiography that render it less effective in some cases; problems due to projection geometry, contrast changes, and superimpositions of anatomical structures are the three most influential factors. The problems with contrast changes are the easiest to solve [6].
Several studies have evaluated different radiologic methods for assessment of bone level in periodontal diseases. These studies have suggested that bitewing radiography is the second best option for the detection of the alveolar bone level changes after parallel radiography. In bitewing radiography, the film is almost parallel to the long axis of the interdental bone, so the geometric distortion is minimized in this method [7,8,9]. Several studies have shown the advantages of digital radiography in diagnosis of periodontal disease and assessment of alveolar bone level [10,11,12].
The improvement of radiographs in detection of periodontal diseases and bone defects by making contrast changes has also been assessed [13,14,15]. Benn [16] improved dental radiographs by decreasing the exposure dose. They showed that decreased beam expansion and retraction of the cheek are more effective in rendering radiographs with better contrast for evaluating bone level. The reliability of radiographs in the detection of periodontal diseases and measurement of alveolar bone loss has been evaluated [17]. Bohay [17] determined the percent accuracy, sensitivity, specificity, and reliability of periapical radiographic diagnosis of periodontal diseases. In their study, Specificity of periapical radiographic diagnosis is higher than sensitivity.
The exposure time can be decreased by retracting the buccal soft tissues; thus, the exposure dose of the patient can be reduced while the contrast of the radiographs will be increased [16]. This study aims to assess the accuracy and reliability of premolar bitewing radiographs taken while retracting the cheeks for evaluation of the interdental bone level.
MATERIALS AND METHODS
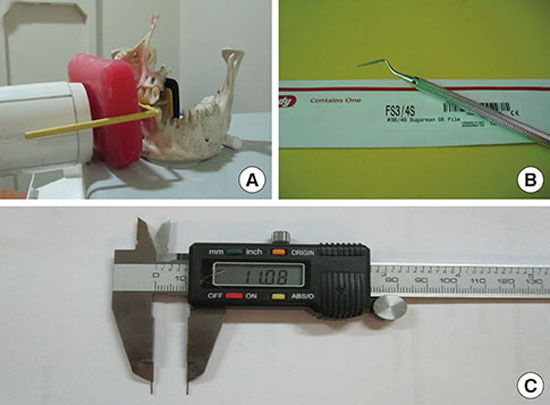
This diagnostic laboratory study was designed and performed at School of Dentistry, Shahid Beheshti University of Medical Sciences, in 2013. This study was executed on 3 dried maxillae and mandibles (a total of 6 bones and 12 quadrants). Seventy-two interdental horizontal bone defects in the area of the premolars were created on the dried bones by a 3S/4S Sugarman DE file (Hu-Friedy, Chicago, IL, USA). The depth of the defects was measured from the cement-enamel junction (CEJ) at the buccal, middle portion and lingual aspects of the teeth via a digital caliper (Mitutoyo, Aurora, IL, USA) and the lowest measurements were recorded (Fig. 1). The digital caliper was used to measure the length of a 10-cm ruler repeated 10 times to prove the reliability of the caliper, and it showed the same 10-cm measurement every time. All measurements were taken by a blinded expert periodontist with 93% reproducibility. After creating the defects, digital bitewing radiographs were taken by photostimulable phosphor plates (PSP No.2, Soredex, Tuusula, Finland) and a Minray intraoral x-ray unit (Soredex) at 70 kVp and 8 mA settings. A rose wax with 20 mm thickness was used as a soft tissue simulator. The radiographs were divided into three groups:
Each group was divided into six subcategories: Defects in the distal aspect of the canines, the mesial aspect of the first premolars, the distal aspect of the first premolars, the mesial aspect of the second premolars, the distal aspect of the second premolars, and the mesial aspect of the first molars. There was one radiograph obtained in each defect area (i.e., a total of 12 radiographs in each subcategory and 72 in every main group). The radiographs were processed with DIGORA software ver. 2.6 (Soredex). The overall reliability of the software has been demonstrated by the company [18]. The distance between the CEJ and the alveolar crest was measured by an oral and maxillofacial radiologist and recorded as the radiographic depth of the alveolar bone defects (Fig. 2). The radiologist was unaware of the radiography groups (single-blind study).
Statistical analysis
All calculations were processed using IBM SPSS Statistics ver. 20.0 (IBM Co., Armonk, NY, USA). Descriptive statistics including tables and graphs were used to document the information. The validity and reliability of each radiography technique were assessed. In this study, the measures were the amount of alveolar bone loss detectable in the bitewing radiographs. In order to assess the reliability of different techniques, an exact type ICC test with a 95% confidence interval was performed [19]. A P-value of less than 0.01 was considered statistically significant. Analysis of variance (ANOVA) was used to assess the validity of the techniques and a P-value less than 0.05 was considered statistically significant [20].
RESULTS
We assessed the reliability of radiographs by checking the agreement on measurements among the radiographs within each group by using ICC. The results of ICC analysis are shown in Table 1. This study shows that although all three radiography techniques were reliable, the radiographs taken with 0.16 second exposure time and without a soft tissue simulator (group 3) were more accurate and reliable than the others (ICC=0.96, P<0.001).
In order to assess the validity of radiography techniques, ANOVA was used to compare the radiologic measurements with laboratory (actual) measurements on dried bones (gold standard). The results are shown in Table 2. The radiographs taken with 0.16 second exposure time and without a soft tissue simulator (group 3) had higher validity than the other two groups except for the mesial and distal aspects of the first premolars, although these findings were not statistically significant (P=0.6). The radiologic measurements of the defects on the mesial aspect of the second premolars were closer to the gold standard than those of the other radiographs. The radiologic measurements of the defects at the distal aspect of the canines were much different from the gold standard (2.92 vs. 3.35).
DISCUSSION
In the current study, we evaluated the efficacy of a new radiography method that can be used in a radiography unit for detection of interdental alveolar bone defects on bitewing radiographs. We retracted the cheek soft tissue with a retractor and reduced the exposure time when taking the radiographs. We used a 20-mm rose wax to simulate soft tissue in the laboratory [21]. Reducing the exposure time leads to a decrease in the exposure dose of the patient and results in less severe biological aspect effects of radiation for patients. By reducing the exposure time, the contrast of the radiographs will increase. Increased contrast leads to radiologic measurements greater than the actual measure of the alveolar defect. In our study, we used this fact to approximate our radiologic measurements to the clinical depth of the defects. Actual defects visible on the radiographs were smaller than the clinical size; thus, we tried to increase the accuracy of the radiologic measurements by retracting the soft tissue in order to increase the contrast.
All radiographs were divided into three groups. The reliability and validity of the radiographs increased with reduced exposure time and retraction of soft tissue. We compared the case group with two control groups. The first control group received the standard bitewing radiography protocol with 0.2-second exposure time with the presence of soft tissue. In the second control group, the exposure time was similar to the case group (0.16 second) with the presence of soft tissue. This study design was based on the concept that with retraction of the soft tissue and reducing the exposure time, the reliability and validity of the radiographs would increase.
The main advantage of this study over the previous ones [22,23] is that we used dried bones to create bone defects and measured the depth of the alveolar defects by a digital caliper with an accuracy of 0.01 mm, whereas other studies [22,23] measured it via a periodontal probe with an accuracy of 1 mm. We used digital radiography and DIGORA software with an accuracy of 0.0359 mm for radiologic measurements.
Benn [16] demonstrated that elimination of soft tissue improves the detection and detail presentation of alveolar bone defects on radiographs. They used periapical radiography with the parallel technique to detect the defects. They concluded that the elimination of soft tissue improves the contrast of the radiographs. Their findings were similar to the results of our study.
The closest results of radiologic measurements to the clinical findings were observed at the mesial aspect of the second premolar tooth. The greatest difference was seen at the distal aspect of the canines. This study suggests that, of the three methods we evaluated, the bitewing radiography with reduced exposure time and the retraction method may be most useful and have the best results in measurement of the interdental alveolar bone level between premolars. These findings were in contrast to the results of Albandar et al. [24]. They concluded that bitewing radiographs show higher proportions of unreadable sites in the canines and the mesial surface of the first premolars than periapical radiographs [24].
The limitations of the present investigation were that we ignored the absence of gingival tissue on dried bones and we only evaluated this method in horizontal defects. This radiologic method may not be as useful for detecting the vertical and angular bone defects with high reliability and validity. Although new radiography methods like cone-beam computed tomography have been suggested to detect the bone loss in the literature, their superiority to bitewing radiographs has not been proven [25,26,27]. Several investigations have shown the advantage of digital radiography for diagnosis of periodontal defects [28,29,30]. We used digital bitewing radiography to assess the alveolar bone loss because it is easier to retract the soft tissue and place the film in the correct position at the same time than when performing parallel periapical radiography.
In conclusion, the reliability of radiographs with retraction of soft tissue may be higher than other radiography methods for detection of interproximal horizontal alveolar bone loss. Elimination of the buccal soft tissue in digital bitewing radiography may be more important than increasing the exposure time. Digital bitewing radiography with retraction of soft tissue and decreased exposure time may be an appropriate approach for diagnosis of alveolar bone loss in the interproximal region of the premolars.




 XML Download
XML Download