

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Combination therapy is always performed on patients with head and neck cancer. Approximately 60%-80% of patients receive radiotherapy after surgery [1]. To increase their quality of life, restorative treatment is necessary. Among the different restorative methods, implants are widely chosen for their good functional recovery and aesthetic effects [2]. However, radiotherapy leads to a considerable number of difficulties in implant treatment. For example, the tissue in the irradiated area usually leads to a reduction of the vascular portion and cells and to hypoxia [3-5]. These changes lead to the destruction of osteoblasts and impaired bone modelling and remodelling which even cause osteoradionecrosis (ORN) [6,7]. Meanwhile, the radiotherapy may cause reduced saliva secretion and an imbalance of the peri-implant flora [8]. All these factors increase the risk of implant failure. To solve this problem, many strategies have been used in clinical practice, and some have achieved ideal effects. This review mainly focuses on the success rate of implants, tissue changes after radiotherapy, and effective adjuvant therapy methods, including hyperbaric oxygen (HBO), osteogenic growth peptide (OGP), and bone morphogenetic protein (BMP). The aim is to provide a useful guide to improve the success rate of implants in head and neck cancer patients after radiotherapy.
SUCCESS RATE OF IMPLANTS IN PATIENTS WITH RADIOTHERAPY
Radiotherapy is an important factor linked to implant failure. Studies from both animal subjects and human patients indicate that an irradiated bone has a greater risk of implant failure than a nonirradiated bone. This increase in risk may be up to 12 times greater [9,10]. There is much variation in the success rate reported amongst these data. A success rate as high as 99% in the mandible was reported by Keller et al. [11] in patients who had received radiotherapy, whereas rates as low as 70% were reported by Babin et al. [12]. A similar variation is seen in implants placed in the maxilla. The reported success rates vary from as high as 100% to as low as 40%. Buddula et al. [13] analyzed 48 patients who had prior head and neck radiation and had 271 dental implants, and reported that the 3-year survival rate was 238 implants (87.8%). Similar research was performed by Mancha et al. [14]; according to them, the overall 5-year survival rate in irradiated patients was 92.6%. Irradiated patients had a marginally significantly higher implant loss than nonirradiated patients. More importantly, they reported that the 5-year survival rate in the ORN group was only 48.3%. Recently, Linsen et al. [15] showed long-term results of implants following radical head and neck cancer surgery with adjuvant radiation therapy, and the overall 1-, 5-, and 10-year survival rates of all implants were 96.6%, 96.6%, and 86.9%, respectively. Based on the results of the research mentioned above, it was concluded that radiotherapy was the essential cause of implant failure. Irradiation can produce both early and late tissue changes. Early effects include those on the salivary glands, skin, and oral mucosa, whereas later effects involve bone changes leading to demineralization, fibrosis, increased susceptibility to infection, and finally, avascular necrosis [16-18]. Thus, the treatments against the changes in the soft and hard tissues after radiotherapy are meaningful for the success of dental implants in patients with head and neck cancer.
CONSEQUENCES OF RADIATION-INDUCED CHANGES IN TISSUES
Both hard and soft tissues changed when the patients received radiotherapy. These changes are harmful to the restoration and the survival of implants. The radiotherapy could directly injure the remodeling system of the bone, including osteocytes, osteoblasts, and osteoclasts [19]. Meanwhile, it could also cause irradiation-induced vascular injury. Radiation injury to the fine vasculature of bone and its surrounding tissues first leads to hyperemia, followed by endarteritis, thrombosis, and a progressive occlusion and obliteration of small vessels, which would lead to a further cell number reduction and progressive fibrosis in bones [20,21]. All these changes further result in a significant loss of active osteoblasts and osteoclasts as well as periosteal fibrosis and the loss of remodeling elements.
The most severe potential complication of bone irradiation is ORN, which is considered to be an infectious process with compromised vascularity and minimal regenerative capabilities [22]. It usually occurs in the mandible and causes chronic pain and surface ulceration. The incidence of ORN of the mandible varies from 5% to 15%, and the incidence of ORN of the maxilla is much lower. ORN is closely associated with the implantation failure rate [23]. Mancha et al. [14] studied 225 implants placed in 30 patients who had received radiotherapy, and reported that irradiated patients had a marginally significantly higher implant loss than nonirradiated patients. The 5-year survival rate in the ORN group was 48.3% and that in the non-ORN group was 92.3%, with a statistically significant difference between both groups.
Besides the bones, the condition of the periodontium is directly related to the success and survival rate of the implants [24]. The cells and the vascular portion of the periodontal membrane decreased and the periodontal space widened after the patients received irradiation. The radiation-related changes in the cementum and the periodontal ligament may induce infection and increase the risk of hyposalivation, plaque accumulation, and the shift of oral microflora [25,26]. The effects of radiotherapy on the periodontium result in an increased risk of periodontal attachment loss as well as an increased risk of ORN development [27,28].
The change in salivary glands is another important factor that affects the survival rate of the implants. Radiotherapy could lead to a chronic salivary gland dysfunction, which is characterized by a reduced salivary flow and changes in the saliva composition [29]. The affected patients suffered from xerostomia, oral mucositis, difficulty in speaking, increase in oral pathologies, difficulty in chewing and swallowing food, and malnutrition due to a loss of the salivary flow [30,31]. Overall, these changes would destroy the environment of the oral cavity and ultimately, decrease the survival rate of the implants.
Radiotherapy causes different levels of damage to oral health. In addition to the changes in the hard and soft tissues in the oral cavity mentioned above, the damage of the oral mucosa, radiation caries, periodontal disease, dysfunction of muscles and joints, and imbalance of the nutritional status would all increase the risk of implant failure [32-35]. Thus, prevention and treatment considerations for irradiated patients are essential to improve the implant survival rate.
STRATEGIES FOR IMPROVING THE SURVIVAL RATE OF IMPLANTS IN IRRADIATED PATIENTS WITH HEAD AND NECK CANCERS
Hyperbaric oxygen
HBO therapy is a treatment modality in which a person breathes 100% O2 while exposed to increased atmospheric pressure [36]. It is the most studied and the most widely used therapy for improving the implant survival rate after radiotherapy adjuvant therapy. HBO therapy has been successfully used in the treatment of several disorders caused by tissue hypoxia, due to the extraoxygen supply to the tissues that it enables. For the bones after radiotherapy, HBO can cooperate with the basic fibroblast growth factor (bFGF) and protect the bone and bone marrow [37]. For the tissue damage after radiotherapy, HBO can improve the implant survival rate and achieve the ideal efficacy [38]. Granstrom et al. [39] retrospectively evaluated the implant survival of 631 implants installed in irradiated cancer patients over a 25-year period. The implant failure rate in HBO-treated patients was 8.5%, compared with the 40.2% of the non-HBO-treated group. In mouse models, it was found that HBO had significant effects on the treatment of irradiated tissues [40]. Through the study of histology and morphology, they found that HBO treatment could increase the formation of bone trabecular and bone exposure. In the irradiation region, HBO could significantly increase the velocity of blood flow. In addition, HBO is a good application for the treatment of ORN, hypo-salivation, radiation caries, and pain initiated by radiotherapy. Thus, HBO therapy can be considered an effective therapy for the prevention or treatment of the long-term complications of radiation therapy [41,42].
However, it has been insisted that HBO is not necessary in improving the survival rate of dental implants placed in irradiated bone because the incidence of ORN was very low (approximately 5%) and ideal survival rate of the implants could be achieved with prolonged healing period in previous studies. More importantly, HBO has some contraindications, including optic neuritis, pulmonary disease, claustrophobia, and epilepsy [43,44]. Correspondingly, the use of HBO can cause some complications, such as dysfunction of the eustachian tube, periosteal rupture, seizures, and decompression sickness [45,46]. In summary, HBO therapy has the potential to improve the implantation survival rate of patients received radiotherapy; however, the timing and indications for the use of HBO therapy should be in accord with specific conditions clinically.
Bone morphogenetic proteins
BMPs are a group of growth factors known as cytokines and metabologens. Originally discovered by their ability to induce the formation of bone and cartilage, BMPs are now considered to constitute a group of pivotal morphogenetic signals, orchestrating tissue architecture throughout the body. These molecules primarily stimulate the differentiation of mesenchymal stem cells into chondroblasts and osteoblasts; they may contribute to the improvement in periodontal regenerative outcomes and are important for bone formation and renewal [47]. Wurzler et al. [48] reported that BMP had potential applications in reconstructive craninomaxillofacial surgery after irradiation for it could overcome the radiation-induced impairment of calvarial repair. Springer et al. [49] studied the application of BMP in the irradiated mandible and found that BMP could cooperate with bFGF and result in predictable bone generation. Other studies also identified that BMP could enhance the generation and repair of bones after radiotherapy [50,51].
In clinical applications, BMPs for clinical use are produced using recombinant DNA technology (recombinant human BMPs [rhBMPs]). rhBMP-2 and rhBMP-7 have been shown in clinical studies to be beneficial in the treatment of a variety of bone-related conditions, including spinal fusions and nonunions. In 2001, the U.S. Food and Drug Administration (FDA) approved rhBMP-7 (aka OP-1; Stryker Biotech, Hopkinton, MA, USA) for a humanitarian device exemption as an alternative to autograft in long bone nonunions. In 2004, the humanitarian device exemption was extended as an alternative to autograft for posterolateral fusion [52]. In 2002, rhBMP-2 (Infuse, Medtronic Inc., Minneapolis, MN, USA) was approved for anterior lumbar interbody fusions with a lumbar fusion device. In 2008, it was approved to repair posterolateral lumbar pseudarthrosis and open tibia shaft fractures with intramedullary nail fixation. In these products, BMPs are delivered to the site of the fracture by being incorporated into a bone implant and released gradually to allow bone formation, as the growth stimulation by BMPs must be localized and sustained for some weeks. The BMPs are eluted through a purified collagen matrix that is implanted in the site of the fracture. rhBMP-2 helps to grow bones better than any other rhBMP; therefore, it is considerably more widely used clinically. BMPs could promote and accelerate the new bone formation and maturation in the implant-bone interface [53,54]. Therefore, the use of the exogenous BMP bone tissue may improve the local content and the activity of BMP, and improve the implant survival rate after radiotherapy. Bovine BMP (bBMP) has been shown to increase the rate of osseointegration around cylindrical uncoated endosseous implants, as evidenced histomorphometrically four weeks after implantation in a dog model. The results revealed abundant lamellar bone formation around bBMP-coated implants. This bone was found adjacent to the implant threads and frequently entered the implant holes [55]. In a recent study, combined adenovirus-mediated human BMP-2 gene-modified bone marrow stromal cells with allograft enhanced the defect healing and improved the strength of implant fixation with osseointegration in a 3-mm bone defect around a titanium alloy implant [56].
Osteogenic growth peptide
The OGP is a 14-mer bone cell mitogen that increases bone formation and trabecular bone density and stimulates fracture healing. The overexpression of OGP has a markedly increased peak bone mass [57]. OGP is present in mammalian serum in micromolar concentrations mainly complexed to 2-macroglobulin. Upon its dissociation from the complex, it is proteolytically activated yielding the mitogenic C-terminal pentapeptide OGP [58]. In addition to stimulating bone formation, OGP potently enhances hematopoiesis. We have reported recently that the mitogenic action of OGP involves the activation of a Gi protein-MAP kinase signaling pathway [59]. Gurevitch et al. [60] reported that OGP could increase blood and bone marrow cellularity and enhance the engraftment of bone marrow transplants in irradiated mice. Other animal experiments showed that OGP could induce the transformation of cartilage callus into bone callus at the fracture site, promote the differentiation and maturation of the bone cells around implants, and accelerate the process of osseointegration [61,62]. However, at present, the research on OGP is still limited in terms of animal experiments, and the clinical applications of OGP need further study.
CONCLUSION
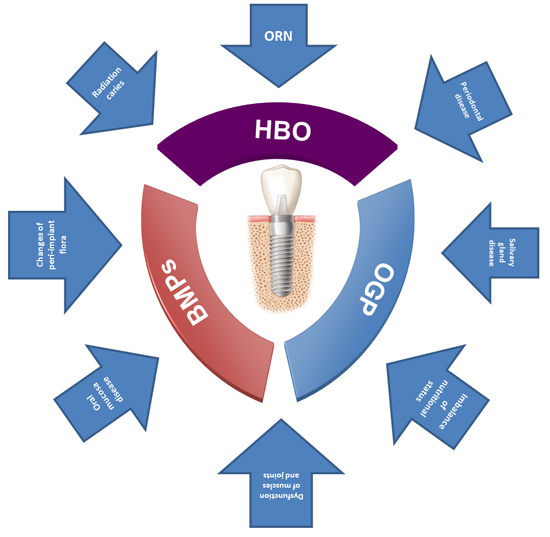
For patients with head and neck cancers, both combination therapy for the tumor and the follow-up implantation for functional reconstruction are necessary. Although radiotherapy is commonly applied to the cancerous tumor as an important means of therapy, it can cause various changes in both hard and soft tissues. All these changes are harmful to implant survival. Based on recent studies, some strategies, such as the use of HBO, BMPs, and OGP, might improve the implant survival rate (Fig. 1). However, every method has its limitations, and the applications and risks of different methods should be discussed further. Thus, the exploration of suitable ways to improve the retention of implants after radiotherapy needs further study.

 XML Download
XML Download