

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The ultimate goal of periodontal therapy is the regeneration of the lost periodontium affected by periodontitis. However, conventional periodontal therapies usually result in tissue repair by the long junctional epithelium rather than true regeneration, that is, the formation of new cementum, new periodontal ligament and new bone [1,2]. Melcher [3] suggested that periodontal ligament cells have the capacity to regenerate the periodontal attachment [4,5]. Associated animal and human studies have established that the occlusion of cells originating from epithelium and gingival connective tissue using tissue barriers is very important in achieving periodontal regeneration [6,7].
Membranes used for the guided tissue regeneration (GTR) procedure should meet the following requirements [8]: biocompatibility, cell occlusion, integration by the host tissues, clinical manageability, and the space-making function. Nonresorbable membranes like expanded polytetrafluorethylene were quite successful in GTR therapy [9]. However, nonresorbable membranes have drawbacks, such as frequent membrane exposure and the necessity of a second surgery for membrane removal. Therefore, several resorbable membranes have been developed to overcome these drawbacks and are now widely used for guided tissue or bone regeneration [10,11].
Collagen membranes are selected frequently from the various available resorbable membranes because they have many advantageous properties including a low immune response, low toxicity, the ability to promote cellular growth and attachment, homeostasis, and the ability of collagen solutions to reconstitute into the microfibrillar structure found in natural tissues [12,13]. Nevertheless, collagen membranes are absorbed too quickly to maintain structural integrity during bone/tissue regeneration. Various physical and chemical cross-linking techniques have been applied to control the rate of collagen biodegradation, such as ultraviolet light, glutaraldehyde, and enzymatic activity. [14]. One such technique, glucose-mediated cross-linking, is a method that uses natural processes occurring in the body, and therefore may be more biocompatible than other methods [15,16]. Lee et al. [17] reported that a porous nonchemical (glucose) cross-linking collagen membrane was able to enhance bone regeneration in an animal study. However, no randomized clinical trial study was carried out to investigate the efficacy of nonchemical cross-linking collagen membranes in treating intrabony periodontal defects. A bioresorbable bilayer collagen membrane (BC) has demonstrated its potential to promote periodontal regeneration in several studies and clinical trials [18,19].
Therefore, the purpose of this randomized clinical trial was to assess and compare the clinical and radiographic outcomes of GTR therapy to treat human periodontal intrabony defects with two different collagen membranes: a nonchemical cross-linking collagen membrane and a frequently used type of BC, in combination with bovine bone mineral (BM).
MATERIALS AND METHODS
Subjects
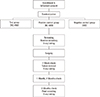
Thirty periodontitis patients who visited the Department of Periodontology, Wonkwang University Daejeon Dental Hospital, Wonkwang University School of Dentistry from October 2012 to October 2013 were enrolled in this study. Each patient was given a detailed description of the procedure and was required to sign an informed consent from prior to participation. The study protocol was approved by the Institutional Review Board of Wonkwang University Dental Hospital (IRB No. W-1202/004-005). The inclusion criteria were: (1) age between 18 and 65 and approval for surgical treatment, (2) the presence of a bone defect of more than 4 mm and probing depth over 6 mm, and (3) agreement to participate in the trial and presence of a signed consent form. The exclusion criteria were: (1) the presence of an acute abscess, (2) pregnancy or breastfeeding, (3) the presence of an orthodontic appliance, and (4) ethical issues that led to the judgment that it would be inappropriate for a given patient to participate in the clinical trial. There was a total of 30 patients, who were randomized among the three groups. To ensure randomization, we used a computer-generated randomized allocation table. There were 10 patients in the positive control group (BC+BM), which was treated with a BC (Bio-Gide, Geistilich, Wolhusen, Swiss) and a xenograft (OCS-B, NIBEC, Jincheon, Korea), and 10 patients in the test group (NC+BM), which was treated with a porous nonchemical cross-linking collagen membrane (NC) (GuidOss, NIBEC) and a xenograft (OCS-B, NIBEC). In the negative control group (BM), the 10 patients were treated with xenograft only (OCS-B, NIBEC). The flow chart of the study is shown in Fig. 1.
Clinical examinations
A blinded single examiner performed all measurements. Examiner reliability was assessed by re-examining 10 randomly selected patients with an interval of 10 days between measurements. A 98% agreement within 1 mm was achieved.
The following clinical measurements were made at baseline and at 3 months after surgery: plaque index (PI), gingival index (GI) [20], probing pocket depth (PD), gingival recession (GR), and clinical attachment level (CAL). The measurements were made at 6 sites per tooth. The PD was measured from the free gingiva to the pocket base. The cemento-enamel junction (CEJ) was used as a fixed reference for the GR measurement. The CAL was defined as the sum of the depth of the pocket and the GR. All examinations were performed using a periodontal probe (PW, Hu-Friedy Manufacturing Co., Chicago, IL, USA).
Radiographic analysis
Standardized radiographs using the paralleling technique with a plastic film holder (XCP, Rinn Co., Elgin, IL, USA) were taken at baseline, 1 week, and 3 months after surgery. The variables were measured as follows: (1) the distance between the radiographic projection of the CEJ and the bottom of the defect was measured (CEJ-BD), (2) the distance between the radiographic projection of the CEJ and the alveolar crest was measured (CEJ-AC), (3) the radiographic bone fill was calculated as the difference between baseline CEJ-BD and 3 months CEJ-BD, and (4) the change in the radiographic bone level after surgery was estimated as the difference compared 1 week with 3 months for CEJ-BD and CEJ-AC, respectively (Fig. 2). The radiographs were analyzed using the PiView system (PiView STAR, Infinitt Co., Seoul, Korea).
Surgical procedure
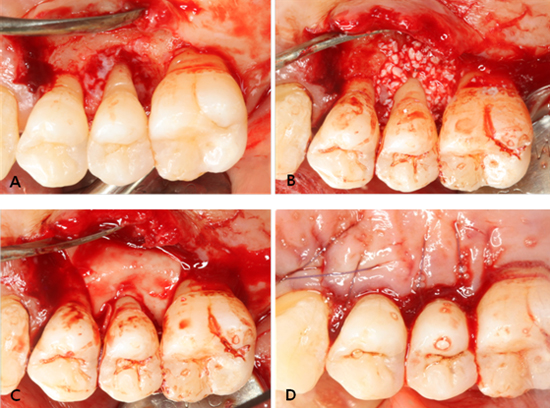
All operative procedures were performed under local anesthesia by a single surgeon. Following intracrevicular incisions, full-thickness mucoperiosteal flaps were raised vestibularly and lingually. All granulation tissue was removed from the defects and the roots were thoroughly scaled and planed using hand and ultrasonic instruments. After the surgical site was prepared, a xenograft was applied on the defect. A bioresorbable membrane was trimmed and adapted over the defect in such a manner that the entire defect and 2-3 mm of the surrounding alveolar bone were completely covered. The membrane was not sutured. The flaps were repositioned and sutured in a slightly coronally displaced position. All patients received antibiotics and analgesics for 5 days (375-mg amoxicillin and 60-mg loxoprofen). The postoperative care consisted of 0.2% chlorhexidine digluconate solution rinses twice a day for 6 weeks. Recall appointments were scheduled during the remaining observation period. Pathological tissue alterations, device exposure, or other pertinent clinical observations related to the surgery were recorded. Clinical photography was used to document the defects and progression of healing (Fig. 3).
Statistical analysis
An estimate was made of the sample size from each experimental group needed to detect a radiographic bone fill difference of 1.5±1.2 mm between treatments with a significance level of 5% and a power of 80%. An estimated 20% dropout was allowed in the final sample size calculation (n=10). The data analysis was performed using SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA). The comparison of the gender proportion between groups was performed using a chi-square test. A one way analysis of variance test with 95% confidence intervals was used to identify statistically significant differences in clinical parameters and radiographic changes among the three treatment groups. Comparisons between baseline data and data from the 3-month follow-up in the test and control groups were made using the paired t-test (α=0.05).
RESULTS
Thirty subjects completed the study protocol; 20 subjects received the GTR/bone graft combination (the test and positive control groups) and 10 subjects received the bone grafting control protocol. There were no relevant differences between the test and control groups involving gender and age distribution (Table 1). Complete gingival wound closure for primary intention healing was accomplished for all defect sites. Membrane exposure was not observed in any cases. No other adverse reactions or relevant clinical findings other than GR were observed.
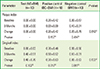
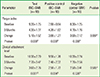
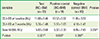
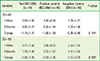
The mean values of clinical parameters including PI, GI, PD, and CAL at baseline and 3 months after surgery are shown in Tables 2 and 3. There was no significant change in PI or GI compared to baseline in any treatment groups. The probing depth reduction for the NC+BM, BC+BM, and BM groups was 5.10±1.52, 3.60±1.27, and 3.60±2.12 mm, respectively. Clinical attachment level gains were 3.60±2.76, 2.50±1.72, and 2.50±3.41 mm for the NC+BM, BC+BM, and BM groups, respectively. Both the PD and CAL improved significantly compared to baseline (P<0.05) in all 3 groups at 3 months after surgery. However, there were no statistically significant differences in PD reduction or CAL gain (P>0.05) between the 3 treatment groups (Table 3). The radiographic mean bone fill was 5.83±3.68, 5.02±2.39, and 6.95±2.43 mm for the NC+BM, BC+BM, and BM groups, respectively. Although the radiographic bone fill was statistically significant compared to baseline (P<0.05) in both the test and control groups, the difference of radiographic bone fill between the treatment groups was not statistically significant (Table 4). The changes in the radiographic alveolar crest level (CEJ-AC) and the bottom level of the defect (CEJ-BD) between 1 week and 3 months after surgery are presented in Table 5. There was no statistically significant difference in bone level change between the test and control groups.
DISCUSSION
In the present study, we clinically assessed and compared the efficacy of GTR therapy using NC collagen and BC collagen membranes in combination with a xenograft for the treatment of intrabony defects. Both collagen membranes (NC and BC) were comparable in terms of pocket depth reduction and gain of CAL. We could not ascertain whether the clinical improvement was due to tissue regeneration, repair, and/or a combination of both healing events because a histological study was not performed. Histometric studies in animals and humans provide evidence that GTR surgery using biodegradable barriers is likely to result in the establishment of a new connective tissue attachment [6,21].
An animal experiment has shown that collagen membranes potentially lead to bone regeneration [22]. Furthermore, human case studies and controlled clinical studies have been presented describing the successful use of collagen membranes in the GBR procedure [23,24]. Various bone graft materials have been used discretely or in combination with GTR to support the regeneration of periodontal tissues. The application of a bone graft produced considerably variable outcomes [25]. In this study, the radiographic bone fill was statistically significant compared to baseline in all treatment groups without a significant difference between the test and control groups. In the evaluation of periodontal regeneration, the formation of new periodontal attachment and the formation of new bone have to be separately evaluated, since they seem to be unrelated events [26]. A GTR device (a porous nonchemical cross-linking membrane) was evaluated previously in one-wall intrabony defects in beagle dogs [17]. In that animal study, new bone height was greater in the membrane-covered group compared to the control group, which did not have a membrane. However, for parameters dealing with the regeneration of periodontal tissue, including junctional epithelium migration and new cementum height, there were no statistically significant differences between the two groups.
The present study demonstrated clinical improvements similar to those reported for several other treatment strategies, including biologic mediators such as platelet derived growth factor, autogenous bone grafts, bone biomaterials, enamel matrix derivates, and GTR as discrete protocols or in combinations [27,28]. The variation in outcomes may be related to defect location and configuration, surgical technique, postsurgery protocol, evaluation method, and the presentation of the data. Only deep intrabony defects seemed to have a substantial clinical regenerative potential in absolute measures [29]. Thus, direct side-by-side comparisons of treatment effects between studies may not be entirely meaningful in the present and other settings.
Wound failure including membrane exposure is a disaster in periodontal-regenerative therapy utilizing the GTR technique because it makes the procedure unpredictable in clinical practice [27,30]. Trombelli et al. [30] demonstrated the clinical significance of wound closure in a retrospective evaluation of GTR therapy. The increase in probing bone level in sites without membrane exposure averaged 4.1±2.3 mm, in contrast to 2.2±2.3 mm in sites with membrane exposure. In this study, complete gingival wound closure was accomplished and membrane exposure was not observed in any cases. The radiographic bone fill was over 5 mm in both the NC and BC groups (Table 4). Bony change indicating resorption of the alveolar crest and grafted BM after GTR/bone graft combination seemed to be independent of the type of the barrier membrane in this study, that is, there was no significant difference in bony change between the NC and BC groups.
Within the limit of this study, NC and BC are comparable in terms of clinical and radiographic outcomes for the treatment of periodontal intrabony defects.
Further investigation is necessary to confirm the influence of NC on periodontal tissue regeneration in light of the small population, short evaluation period, and limited design of this study.



 XML Download
XML Download