

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
C-reactive protein (CRP) is considered to be an important acute phase-sensitive marker of infectious burden and/or inflammation, and is the best indicator of an individual's systemic inflammatory status [1]. Studies have suggested that CRP serum concentrations in the upper quartiles of normality have a considerable role as predictors for future coronary events in healthy populations. Furthermore, low-grade infections with their moderate acute-phase reactions may accelerate the risk of cardiovascular events [1,2].
Chronic periodontitis, an inflammatory disease of tooth-supporting structures, results in the loss of periodontal support, with increased tooth mobility and eventually tooth loss [3]. Investigations have further suggested that patients with chronic periodontitis present with increased systemic inflammation and raised levels of various inflammatory markers when compared with those in unaffected control populations [4]. Although CRP is mainly produced by the liver, it has also been reported to be produced by adipocytes, vascular smooth cells and gingival tissues in response to a rise in interleukin 6 (IL-6) and tumor necrosis factor alpha (TNF-α) [5]. Thus, CRP has been considered to be a possible mediator of the relationship between periodontitis and systemic conditions [6].
The chronic metabolic disorder diabetes mellitus is a serious global health problem of epidemic magnitude. Type 2 (noninsulin dependent or adult-onset) diabetes mellitus, is characterised by defective insulin secretion and action [7,8]. It doubles the incidence and severity of chronic periodontitis [9], and conversely, the presence of periodontitis may also negatively impact the cardio-vascular risk status in type 2 diabetes mellitus (T2DM) patients [10]. Furthermore, as compared to those without periodontitis, periodontitis patients have elevated levels of resting plasma glucose [11,12]. Several studies have demonstrated an inflated inflammatory response in the monocytes of diabetic patients in response to lipopolysaccharides from gram-negative periodontal pathogens. This leads to the release of large amounts of inflammatory mediators and proinflammatory cytokines such as IL-1β and TNF-α [13]. Moreover, in diseased tissues, as diabetic control decreases, there is an increase in GCF along with IL-1β and gingival inflammation [13].
A possible reduction in the severity of systemic diseases following periodontal therapy due to the reduction in the inflammatory burden, in both systemically compromised patients as well as otherwise healthy individuals, has been reported by many [14,15]. Nonsurgical periodontal therapy (NSPT) may also result in the reduction of glycated hemoglobin (HbA1c) levels in diabetic chronic periodontitis patients [10,16]. CRP levels in gingival crevicular fluid (GCF) and serum increased proportionately with the severity of periodontal diseases [16], and studies have also demonstrated increased serum CRP levels caused by a moderate inflammatory stimulus after periodontal therapy [17]. Thus, the aim of this pilot intervention was to evaluate the impact of scaling and root planing (SRP) on the CRP levels of GCF and serum in chronic periodontitis patients with or without T2DM.
MATERIALS AND METHODS
Study population and experimental design
The study was a prospective, longitudinal, case-controlled intervention trial with a three-month follow-up. The study protocol was approved by the Institutional Human Ethics Committee (No. SDC/IHEC 07/2013), and all the participants received an explanation of the study and gave written informed consent before entering the study. Human participants for the study were recruited from the patients referred to the Department of Periodontology, Saraswati Dental College and Hospital, Lucknow, India. Nonalcoholic, nonsmoking subjects with at least 20 teeth in the oral cavity, a 5-mm or greater probing pocket depth (PPD) and a 3-mm or greater clinical attachment loss (CAL), and established radiographic bone loss, at more than 30% of the sites involved, were included for the study. Patients with a medical history of any systemic disease other than T2DM; on any medication other than hypoglycaemic agents; or who had undergone periodontal treatment over the preceding 6 months and needed prophylactic antibiotics in association with periodontal probing or had tissue necrosis and trauma were excluded. Anamneses and records were carefully analysed to retrieve the data regarding the diabetic and general health status of the patients. Only those T2DM patients who were being treated by either dietary intervention or oral hypoglycaemic agents were included for the study in the experimental group. The subjects with T2DM were not encouraged to make any changes in oral hypoglycaemic medications or physical exercise during the course of the study.
Patients fulfilling the selection criteria were initially screened by measuring vital signs (blood pressure, temperature, respiratory rate and pulse rate), and random blood sugar (RBS) using an automated cell counter (Cell-Tech Junior Hematology Analyzer, Logotech Pvt. Ltd., F.I.E, Patparganj, Delhi, India). Forty-eight participants from a north Indian population with generalised chronic periodontitis agreed to participate voluntarily. Based on the initial screening, the participants were divided into an experimental (T2DM-CP) group (group I, n=24), which included chronic periodontitis with T2DM and RBS≥200 mg/dL, and a control (NDM-CP) group (group II, n=24), which included chronic periodontitis without T2DM and with RBS<200 mg/dL.
Methodology
At baseline, the plaque index (PI) by Silness and Loe [18] and gingival index (GI) by Loe and Silness [19] were recorded. To evaluate systemic and hematologic parameters (total leukocyte count [TLC], neutrophil count [Neutr], lymphocyte count [Lymph], serum CRP, HbA1c, and RBS levels), blood samples were obtained from the venous puncture of the antecubital vein (as explained below). On the subsequent day, supragingival plaque was wiped off, and GCF samples were collected as per the study protocol given by Pradeep et al. [14], and the collected blood and GCF samples were sent to the laboratory for evaluation.
All forty-eight cases were recruited for NSPT at baseline, which included full mouth SRP in a single sitting with subgingival mechanical debridement. Oral hygiene instructions were given, and 0.2% chlorhexidine mouthwash for 2 weeks was prescribed. Patients were recalled at 1 month and 3 months.
Clinical (PI, GI, PPD, and CAL) parameters were recorded at baseline, 1 month, and 3 months. The same investigator recorded all the clinical measurements (PI, GI, PPD, and CAL), throughout the study. The examination included duplicate measurements using a UNC-PCP 15 (Hu-Fridey, Chicago, IL, USA) probe; measurements were rounded to the nearest millimetre. To estimate systemic/hematologic parameters, namely the RBS and HbA1c levels, GCF and blood samples were collected and sent to the laboratory at baseline, 1 month and 3 months.
GCF-CRP analysis (Figs. 1 and 2)
Sample collection
Only one site per patient with maximum PPD and CAL was selected as a sampling site in the chronic periodontitis with T2DM (experimental group I) and chronic periodontitis without T2DM (control group II). The GCF sample was obtained by placing the microcapillary pipette gently at the entrance of the gingival sulcus. The area was isolated using cotton rolls to avoid contamination by saliva. GCF was collected using the calibration on colour-coded white 1- to 5-µL calibrated volumetric microcapillary pipettes (Sigma Aldrich Co., St. Louis, MO, USA). Each sample collection was tested for a maximum of 5 minutes (GCF volume [GCF vol]), and the sites that did not express any GCF within the allotted time were excluded. This was carried out to prevent trauma to the sample. During sample collection, samples contaminated with blood and/or saliva were excluded from the study [14].
Sample transport and storage
The microcapillary pipette containing the sampled GCF was wrapped in foil and placed in a THERMOCOL medicine box (Prakash Packaging, Ghaziabad, Uttar Pradesh, India) containing reusable gel refrigerants and was transported to the laboratory and stored at -70℃ until further processing.
GCF-CRP estimation
The collected GCF sample was then assayed for CRP levels by using a highly sensitive CRP enzyme-linked immunosorbent assay (ELISA) kit (Biotron Diagnostic, Hemet, CA, USA), as per the manufacturer's instruction manual.
Principle of the assay
The high sensitivity CRP-ELISA tests were based on the solid phase ELISA principle. Mouse monoclonal antibody (anti-CRP antibody), as opposed to a distinct antigenic determinant on the CRP molecule, was utilised on the microtitre well for solid-phase immobilization. The antibody (horseradish peroxidase) enzyme conjugate solution contained goat anti-CRP antibody. Simultaneously, the sample to be tested was allowed to react with the two antibodies, resulting in sandwiching of CRP molecules between enzyme-linked and solid phase antibodies. After 45-minute incubation at room temperature, the wells were washed with water to remove unbound labelled antibodies. Then, after adding tetramethylbenzidine (TMB) reagent, the sample was incubated for 20 minutes, which resulted in the development of a blue colour. The development of colour at 450 nm was measured spectrophotometrically.
Reagents and materials
Antibody-coated wells (1 plate, 96 wells) consisting of mouse monoclonal anti-CRP layered microtitre wells were used. A reference standard set (1.0 mL/vial) contained 0 mg/L CRP, 0.005 mg/L CRP, 0.010 mg/L CRP, 0.025 mg/L CRP, 0.050 mg/L CRP, and 0.100 mg/L CRP within phosphate-buffered bovine serum albumin (BSA) solution along with preservatives. hsCRP sample diluent (50 mL/vial) consisted of phosphate-buffered BSA solution along with preservatives. CRP-enzyme conjugate reagent (12 mL/vial) was made from goat anti-CRP conjugated to horseradish peroxidase along with preservatives. TMB reagent (11 mL/bottle) and stop solution (1 bottle, 11 mL/bottle) contained one-step TMB solution and diluted hydrochloric acid (1N HCl), respectively.
Assay procedure
Each patient sample was diluted 100 folds prior to use. The required number of coated wells in the holder was secured. Ten microlitres of CRP standards, diluted samples and diluted controls were dispensed into the appropriate wells. One hundred microlitres of CRP-enzyme conjugate reagent was then dispensed into every well. The reagents were then thoroughly mixed for 30 seconds. Incubation was performed at room temperature (18℃-25℃) for 45 minutes. The incubation mixture was eliminated by flicking the plate contents into a waste box. The microtitre wells were rinsed 5 times and flicked using distilled or deionized water. To remove all the residual water droplets, the wells were struck sharply onto absorbent paper or paper towels. One hundred microlitres of TMB solution was dispensed into each well, gently mixed for 5 seconds and incubated at room temperature for 20 minutes. One hundred microlitres of stop-solution was added to every well to stop the reaction, and then mixed gently for half a minute. When all the blue colour changed to yellow, the absorbance at 450 nm was read within 15 minutes using a microtitre well reader.
Calculation
For each set of reference standards, controls and specimens, the mean absorbance value (OD450) was calculated. By plotting the mean absorbance obtained for each reference standard on the vertical (y)-axis versus its concentration in milligrams per millilitre on the horizontal (x)-axis, a standard curve was constructed on graph paper. The corresponding concentration of CRP (mg/L) was determined for every sample from the standard curve using the mean absorbance value. To obtain CRP results in, milligrams per litre, the values of the control sera and the patient specimens were multiplied by the dilution factor of 100. Further 10-fold dilution after the initial 100-fold dilution (total dilution 1:1,000) was performed in specimens having CRP concentrations greater than 10 mg/L, and to obtain CRP results in mg/L, the final CRP values were multiplied by 1,000.
Glycemic control (HbA1c) and systemic/hematologic marker analysis
To evaluate glycemic control (HbA1c) and systemic/haematological markers, blood samples were obtained from venous puncture of the antecubital vein. Verbal confirmation of fasting status was obtained from participants before clinical sample collection. A tourniquet was tied around the arm of the patient from which the blood had to be drawn. Two venous blood samples (5 mL total volume) were collected from the antecubital vein by venipuncture, using a 20-gauge needle with a 5-mL syringe [20]. One blood sample (3-mL volume) was used to extract serum after being allowed to clot at room temperature for 6o minutes followed by centrifugation for 10 minutes. This serum sample was placed in plastic vials, and to estimate serum CRP, it was sent to the laboratory. The other blood sample (2-mL volume) was placed in a plastic vial containing ethylenediaminetetraacetic acid and was sent to the laboratory for the estimation of HbA1c and systemic/hematologic markers [14]. The serum and blood samples collected were immediately transferred to airtight plastic vials and were placed in a thermocol medicine box (Prakash Packaging, Gaziabad, Uttar Paradesh, India) containing reusable gel refrigerants. The specimens were then transported to the laboratory, where they were stored at -20℃ until further processing.
Estimation of HbA1c
The nephelometry method (Agappe Diagnostics, Ernakulam, Kerala, India) that was used for the HbA1c estimation utilizes the interaction of an antigen with an antibody in whole blood or direct determination of HbA1c. Total hemoglobin and HbA1c have the same nonspecific absorption rate as a latex particle. Antihuman HbA1c monoclonal antibodies from a mouse, when added (R2), resulted in formation of latex HbA1c mouse antihuman HbA1c antibody complex. The amount of agglutination occurring due to the interaction of goat antimouse immunoglobulin G (IgG) polyclonal antibody with the monoclonal antibody, is proportional to the amount of HbA1c absorbed into the latex particles' surface [14].
Reagents and their compositions
HbA1c R1 contained Latex (0.13 w/v) and glycine buffer. HbA1c R2 were made up of glycine buffer, mouse antihuman HbA1c, goat antimouse IgG, monoclonal antibody, polyclonal antibody and stabilizers, while HbA1c R3 contained hemolysis reagent.
The test procedure and the calibration data was provided in a smart card along with the kit. The smart card was inserted into a card reader slot, and the display prompted the researcher to add R1 and the sample. One hundred and eighty microliters R1 and 5-µL sample were pipetted into a cuvette and placed into the cuvette holder. After incubation, the display prompted adding R2. Using an attached sensor pipette, 60-µL R2 was pipetted into the cuvette. The results could be viewed on the display and a printout was made.
Hematologic markers
Hematologic parameters, (TLC and differential leukocyte count [DLC]) were recorded with an automated cell counter (Cell-Tech Junior Hematology Analyzer, Logotech Pvt. Ltd., F.I.E, Patparganj, Delhi, India).
Serum CRP estimation
The collected serum sample was assayed for CRP levels by the turbidimetric method using a CRP Turbilatex kit (Fig. 3). The samples were analysed at the Kshitiz Medical and Diagnostic Clinic, Lucknow, India.
Principle for the estimation of serum CRP
This is a quantitative turbidimetric immunoassay for the measurement of CRP in human serum. CRP in the samples binds to specific anti-CRP antibodies, which have been adsorbed to latex particles and agglutinates. The quantity of CRP in the specimen is proportional to the agglutination. The calibration curve prepared from calibrators of well-known concentrations determines the actual concentration.
Reagents and their composition
CRP Turbilatex R1 contains diluent, Tris buffer and sodium azide; CRP Turbilatex R2 contains CRP-Latex (suspension of particles coated with antihuman CRP) and sodium azide; and CRP calibrator.
Laboratory procedure for the estimation of serum CRP
Two test tubes were taken and labelled as test tube 1 and test tube 2. Nine hundred microliters of reagent 1 (CRP R1) and 100-µL reagent 2 (CRP R2) were added to test tube 1. The reagents were mixed well and then 5 µL of sample was added to test tube 1 and again mixed well. The solution in test tube 1 was aspirated in the semi-auto-analyzer and the absorbance was read immediately (A1) and then after 2 minutes (A2) of sample addition. Similarly, 900-µL reagent 1 (CRP R1) and 100-µL reagent R2 (CRP R2) were added to test tube 2 and mixed well, followed by 5 µL of calibrator and another round of mixing. The solution in test tube 2 was aspirated in the semi-auto-analyzer and the absorbance was again read immediately (A1) and 2 minutes after Calibrator addition (A2).
Statistical analysis
The data recorded were analysed using SPSS ver. 15.0 (SPSS Inc., Chicago, IL, USA). The sample size for each group was less than 30; hence distributions were assessed for normality. Assessment of normality was performed using the Kolmogorov-Smirnov test, and many of the parameters were found to be asymmetric. Between group comparisons were made using the Mann-Whitney U-test, and within-group change was studied using the Wilcoxon signed rank test. The confidence level of the study was kept at 95%; thence a P-value less than 0.05 indicated statistically significant association.
RESULTS
Between group comparison
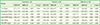
At baseline, group I had significantly lower PI but significantly higher CAL, RBS, and HbA1c mean values as compared to group II (P<0.05). At 1 and 3 months follow-up, mean values for CAL, RBS, and HbA1c were found to be significantly higher in group I in contrast to group II (P<0.05) (Table 1).
At baseline, except for TLC, the mean values for the systemic/hematologic parameters Neutr, Lymph, GCF vol, and GCF-CRP, were nonsignificantly higher for group I (P>0.05). Serum CRP levels were significantly higher in group I as compared to group II (P=0.024). Both at 1 and 3 months, mean values for TLC, Neutr and GCF vol were nonsignificantly higher for group II (P>0.05), whereas serum CRP was significantly higher for group I (P<0.05) (Table 2).
Within-group comparison
Between baseline and 1 month, statistically significant reductions in the mean values of Neutr, Lymph, and GCF vol were observed (P<0.05), whereas, for TLC and GCF-CRP, the reduction in the mean values were nonsignificant for group I subjects (P>0.05). A nonsignificant increase in the mean values of TLC, Lymph, and GCF-CRP (P>0.05), but a significant increase in the mean values of Neutr, and significant reduction in mean values of serum CRP and GCF vol between baseline and 1 month was observed in group II (P<0.05). Between the baseline and 1 month as well as between 1 month and 3 months, a statistically significant reduction in the mean values of TLC, Neutr, Lymph, GCF vol, GCF-CRP, and serum CRP were observed in both groups 1 and II subjects (Tables 3 and 4).
DISCUSSION
Recent evidence shows that patients with periodontitis present with increased systemic inflammation, as indicated by raised serum levels of various inflammatory markers when compared with those in unaffected control populations [4]. Further, the association between periodontal disease and diabetes has also been explored in several studies, and it is widely accepted that more prevalent and severe periodontal disease is observed in persons with diabetes than in nondiabetic persons.
The two-way relationship of periodontal disease with diabetes mellitus is evident with the improvement in metabolic control by the resolution of periodontal inflammation and infection [21]. Systemic inflammatory markers such as CRP, which is an acute phase protein, closely follow the course of inflammation, and hence are used as measure for many disease processes. The available literature has also reported that T2DM patients with chronic periodontitis exhibit clinical improvement after nonsurgical periodontal therapy. However, few studies have reported on the impact of periodontal therapy on CRP levels in GCF and serum, in T2DM patients. Chen et al. [22] reported effective improvement in periodontal and circulating inflammatory status after non-surgical periodontal treatment (NSPT) in patients with T2DM. This study was primarily performed to evaluate the effects of NSPT on the serum and GCF-CRP level in patients with T2DM and chronic periodontitis.
The mean value for PI was significantly higher in group II (NDM-CP) as compared to group I (T2DM-CP), indicating that in spite of having poor plaque control habits, group II (NDM-CP) patients showed less PPD, CAL, GCF vol, and GCF-CRP, as compared to group I (T2DM-CP). This indicates an exaggerated destructive response to dental plaque microorganisms in chronic periodontitis patients with T2DM [10,23].
In accordance with the present study, Kardesler et al. [24] also demonstrated a significant reduction in periodontal health parameters (PI, GI, PPD) at 1 and 3 months after NSPT. CAL levels were significantly decreased at 1 month compared to the baseline values in the well-controlled diabetic patients, while in poorly controlled diabetic patients, there was a slight but nonsignificant decrease in CAL measurements at 3 months [24]. Although the reduction in PI, GI, PPD, CAL, and GCF vol in T2DM patients has been reported by many studies, few studies have reported an effect of SRP on GCF-CRP levels; hence, the significant reduction between baseline and 3 months in GCF-CRP levels could not be corroborated with previously published reports.
There was a significant decrease in all periodontal health parameters except GCF-CRP (PI, GI, PPD, CAL, and GCF vol) between baseline and 1 month, between baseline and 3 months and between 1 and 3 months in group II (NDM-CP) (P<0.05). There was an increase in GCF-CRP levels (0.02±0.08), which was statistically nonsignificant (P=0.076) between baseline and 1 month, but there was a significant reduction in GCF-CRP levels between baseline and 3 months (0.05±0.10), and between 1 and 3 months (0.07±0.10). Similar to our study, Tuter et al. [25] demonstrated that the clinical parameters (PI, GI, PPD) and the GCF vol showed statistically significant reductions in chronic periodontitis patients after SRP with placebo treatment, and SRP with subantimicrobial dose doxycycline (SDD) for 6 weeks. D'Auto et al. [26] suggested short-lived systemic inflammation after periodontal therapy itself, which lasts up to 1 month after the therapy session. As GCF is serum exudate, the levels of GCF-CRP also increase up to 1 month after periodontal therapy session. Further, Megson et al. [27], suggested that CRP in GCF appears to be of systemic origin. Our study reported an increase in GCF-CRP after SRP in chronic periodontitis patients. However, the clinician must understand that once the GCF were collected, and the estimation of CRP levels in GCF are too low to be compared with serum CRP levels. It has also been documented by Megson et al. [27] that the correlation between GCF and serum levels of CRP still requires further investigation before GCF can be considered suitable for the noninvasive assessment of the degree of systemic inflammation in both periodontitis and nonperiodontitis patients.
Similar to the present study, Allen et al. [10] also reported a nonsignificant difference in haematological parameters between an experimental (T2DM-CP) and a control group (NDM-CP) at baseline. Neither the total nor the DLC differed between the two patient groups. Within a single group, both the experimental group (T2DM-CP) and the control group (NDM-CP) showed a significant reduction in white blood cell (WBC) count 3 months after NSPT. A statistically significant reduction in WBC was also reported by two randomized controlled studies, who examined the effects of intensive NSPT on WBC after 6 months [28,29]. Further, Lalla et al. [30] also reported a reduction in the percentage of mononuclear cells (CD14+ monocytes) following periodontal treatment. In accordance with a cross-sectional study of Allen et al. [10], significantly higher levels of serum CRP were detected in T2DM patients with periodontitis as compared with nondiabetic periodontitis. These data agree with reports that diabetes is associated with increased CRP [31] and suggest that periodontitis further augments the CRP levels, when T2DM and periodontitis coexist. An association between serum CRP and periodontitis has been reported in T2DM patients [32], and periodontal therapy reduces serum CRP in T2DM patients [28]. Chen et al. [22] also reported a gradual and significant decrease in serum CRP levels in diabetes mellitus patients with chronic periodontitis from baseline to 3 months after NSPT, which is comparable to the present study (P<0.05). Analogous to the present study, in a control group (NDM-CP), Kamil et al. [33], Ide et al. [34], and Yamazaki et al. [35] all reported that NSPT resulted in a significant reduction in serum CRP levels (P<0.05) in advanced periodontitis patients from baseline to 3 months.
We observed a statistically significant decrease overall in serum CRP levels at 1 month and 3 months after NSPT in group II (NDM-CP) (P=0.027 and P<0.001, respectively). However, out of 24 patients amongst group II, four patients showed a decrease (0.4 to 0.36 mg/L, 4.85 to 1.74 mg/L, 0.89 to 0.87 mg/L, and 2.12 to 1.98 mg/L) in serum CRP levels at one month after NSPT. Amongst these four patients, one patient revealed a baseline serum CRP value of 4.85 mg/L and decrease of serum CRP of 3.11 mg/L at one month. The other 20 patients revealed increases in serum CRP levels at one month that verified the report of D'Aiuto et al. [26], which suggested that periodontal therapy itself results in short-lived systemic inflammation. An important outcome of the our study was that, unlike otherwise systemically health patients in group II (NDM-CP), the gradual decrease in serum CRP levels in these four patients of the group II was similar to the trend shown by group I (T2DM-CP), which may signify some underlying systemic factor that was not reported at baseline by the patient.
An interesting finding in our study was slight (nonsignificant, P=0.076) increase in systemic inflammatory marker CRP in GCF, in group II (NDM-CP) patients at 1 month and then a significant decrease (P=0.002) at 3 months after NSPT. Similarly, for mean RBS, there was an increase at 1 month, and then a decrease after 3 months (P>0.005).
It is well established that T2DM patients have a significantly elevated risk of periodontitis; and periodontitis may exert a converse, negative impact upon cardio-metabolic risk status in type 2 diabetic patients. In chronic periodontitis patients with diabetes mellitus, periodontal destruction occurs due to an exaggerated inflammatory response such as hyperactive neutrophils due to reactive oxygen species production, because of increased oxidative stress and increased insulin resistance [36]. Studies have shown that insulin resistance is increased in the diabetic patient under the influence of local factors, and hence decreases the healing response of tissue. Here, it can be hypothesized that, after NSPT, local factors are removed, leading to a decrease in insulin resistance with a decrease in proinflammatory cytokines (e.g., TNF-α, IL-6) associated with local factors, thus improving insulin sensitivity, ultimately leading to better glycemic control (HbA1c) [37], and in turn, promoting a better wound healing capacity of tissues in T2DM patients. This hypothesis was further validated by a greater decrease in CRP levels (an acute inflammatory marker) in diabetic as compared to nondiabetic patients. Our results showed that CRP levels in both GCF as well as in serum were higher in diabetic chronic periodontitis patients as compared to nondiabetic chronic periodontitis patients. Further, there was a significant improvement in both the groups, but better improvement was observed in diabetic chronic periodontitis patients. As low high-density lipoprotein (HDL) levels, an elevated total cholesterol/HDL ratio and elevated CRP levels are known cardiovascular risk factors, the impact of periodontitis on oxidative stress/inflammatory pathways, insulin production, and cardiovascular health needs to be further explored in T2DM [10]. The consistent reduction in serum CRP levels following periodontal therapy, suggests a probable role for periodontitis in causing systemic inflammation as well as potentially affecting a variety of chronic disorders including cardiovascular diseases and diabetes [5].
Within the limitations of the present study, it can be concluded that CRP levels in both GCF as well as in serum were higher in T2DM-CP patients as compared to NDM-CP patients. NSPT results in statistically significant improvement in periodontal health parameters (PI, GI, PPD, CAL, and GCF vol), CRP levels in both serum and GCF in both group I (T2DM-CP) and group II (NDM-CP). The mean improvement in periodontal health parameters (PI, GI, PPD, CAL, and GCF vol), CRP levels in serum and GCF was greater in group I as compared to group II after NSPT. There was a nonsignificant increase in GCF-CRP, TLC, Lymph, and RBS, and significant increase in Neutr and serum CRP in group II at 1 month. The serum CRP level of 20 out of 24 NDM-CP patients was also increased at 1 month.






 XML Download
XML Download