

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The maxillary anterior region is an esthetically important area. Occasionally, dental surgeons must extract teeth due to advanced periodontal disease, extensive root caries, and/or periapical pathology. After tooth extraction, alveolar bone resorption is inevitable; the ridge tends to decrease by approximately 25% in the first year and 40% is gradually resorbed by the third year [1,2]. The minimum horizontal decrease at the gingival level of an extraction site was reported to be 2 mm [3,4,5]. In the maxillary anterior regions in particular, restorative procedure or implant placement is extremely challenging because of this limitation. To overcome this problem, hard and soft tissue augmentations are occasionally required.
Various bone reconstruction techniques such as block grafts, particulate grafts, ridge expansion techniques, guided bone regeneration (GBR), and distraction osteogenesis have been used for this purpose [6,7,8,9,10,11,12]. The increased bone volume makes achieving primary soft tissue closure difficult, so undermining the flap and displacing it coronally to cover the graft without excessive tension is necessary. However, flap advancement can lead to vestibular height loss and displacement of the mucogingival junction. Thus, the shortened attached gingiva may interfere with the esthetic prosthesis and soft tissue cleansing, especially in the esthetic region. Various flap designs that cover these defects have been described in the literature to correct soft tissue conditions including the connective tissue graft [13,14], palatal advanced flap [15], palatal rotation flap [16,17,18], and buccal fat pad flap [19].
This case report describes the use of a rotated palatal subepithelial connective tissue graft (RPSCTG) procedure to achieve primary soft tissue coverage after GBR and restore the abundant soft tissue volume for an improved esthetic outcome.
CASE DESCRIPTION
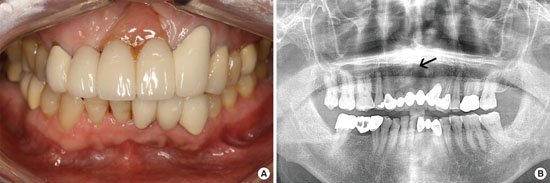
A healthy, 60-year-old man was referred to the Division of Periodontology in the Department of Dentistry at Hanyang University Hospital, Seoul, South Korea, for treatment of an alveolar defect on the anterior maxilla. The patient was partially edentulous in the maxillary arch with an existing fixed partial denture including pink porcelain (Fig. 1A). Radiologic examination revealed a vertical deficiency in the anterior maxilla (Fig. 1B). After removing the prosthesis, clinical examination revealed insufficient hard and soft tissue volume that was classified as Seibert III on the anterior maxillary ridge (Fig. 2A and B) [20]. The patient was dissatisfied with the appearance of the anterior maxillary tissue architecture, so treatment plans were developed to include hard and soft tissue augmentations and a new conventional fixed partial denture.
Surgical technique
Stage 1: GBR and RPSCTG (Left)
Following a mouth rinse with 0.12% chlorhexidine, the operation area was carefully anesthetized using lidocaine. A full-thickness buccal trapezoidal flap was gently reflected with two vertical incisions, whereupon the vertical and horizontal bone defects were observed (Fig. 2C). Following the bone ridge examination, any soft tissue remaining on the alveolar crest was removed with a periodontal curette (Gracey, Hu-Friedy, Chicago, IL, USA). Then, the cortical bone was perforated using a round bur to access bone marrow cells on the graft site. The defects were filled with deproteinized bovine bone mineral (Bio-Oss, Geistlich Pharma, Wolhusen, Switzerland) and were covered with a nonresorbable titanium-reinforced high-density polytetrafluoroethylene membrane (Cytoplast, Re-gentex GBR-200, Ti-250, Osteogenics Biomedical Inc., Lubbock, TX, USA) (Fig. 2D and E). The membrane was fixed with a titanium screw to prevent movement and stabilize a space for bone regeneration (Fig. 2F).
Primary closure could not be achieved by undermining the conventional trapezoidal flap due to the excessive volume of the graft, so a RPSCTG was planned to cover the graft materials. After local anesthesia was administered on the palatal donor site, two parallel palatal incisions were made from the right first molar area to the crestal incision line to obtain pedicled connective tissue. The superficial epithelial flap was reflected with a sharp blade (No. 15) and was retracted posteriorly; subsequently, the deep subepithelial connective tissue flap was elevated and rotated anteriorly to cover the graft site (Fig. 3A-C). To stabilize the RPSCTG, the horizontal mattress sutures were enforced with 5-0 nonresorbable nylon sutures (Ethicon Inc., Somerville, NJ, USA). Additional bioabsorbable sutures (Vicryl 4-0, Polyglactin 910, Ethicon Inc.) were placed above the graft to secure the graft in a tension-free state. In the donor site, the superficial epithelial flap was placed in its original position and sutured (Fig. 3D). Postoperatively, the patient was given amoxicillin plus clavulanic acid (Augmentin, 625 mg, Il-Sung Pharm., Seoul, Korea) 3 times a day for 7 days along with 0.12% chlorhexidine mouth wash. The patient was instructed to refrain from brushing or irritating the surgical area for 4 weeks. The sutures were removed 2 weeks after surgery, and the patient was called for follow-up every 2 weeks after surgery for postoperative care.
Stage 2: Membrane removal and contralateral RPSCTG (Right)
Palatal flap sloughing was observed 2 weeks after the stage 1 surgery (Fig. 4A). Because the membrane was exposed after 4 weeks (Fig. 4B), early membrane removal along with additional soft tissue grafting to cover the exposed bone were planned. The contralateral RPSCTG procedure was performed simultaneously with membrane removal 7 weeks after the stage 1 surgery. An incision was made through the tissue covering the barrier membrane and a full-thickness mucoperiosteal flap was raised. After gentle removal of the exposed membrane, the epithelium remnants on the inner side of the flap were removed. A bioabsorbable collagenous membrane (Bio-Gide, Geistlich Pharma) was applied to cover the bone graft materials. As described above for the stage 1 surgery, the contralateral RPSCTG was rotated and sutured to gain a more abundant soft tissue volume (Fig. 5). These sutures were removed 2 weeks after the stage 2 surgery. The prosthodontic procedure was completed after a 6-month healing period.
Primary coverage was obtained in the stage 1 surgery without tension, but flap necrosis and exposure of the nonresorbable membrane were observed 4 weeks after the stage 1 surgery. Signs of infection or suppuration were not observed in the exposed membrane site. The exposed membrane was managed with chlorhexidine rinsing during the healing period. However, the patient was a heavy smoker and unfortunately did not comply with our request to quit smoking until the end of the treatment period.
The stage 1 surgery enhanced the volume of the soft and hard tissue, and additional soft tissue augmentation was planned in tandem with membrane removal to acquire ideal soft tissue architecture. The nonresorbable membrane was removed and the bone graft materials were covered with a contralateral RPSCTG at 7 weeks postoperatively. Wound healing was uneventful at the graft site with no signs of infection or other problematic symptoms after the stage 2 surgery (Fig. 6). Moreover, palatal donor site healing was uneventful, and epithelization was complete after 3-4 weeks without any complications.
We measured the size of alveolar defect using the study casts. Baseline measurement of the defect revealed a height and width of approximately 13 mm and 5 mm, respectively, whereas a second measurement obtained at 2 months after surgery revealed respective values of approximately 4 mm and 2 mm (Fig. 7). No problems or complications were recorded after 2 months of follow-up (Fig. 8). Six months later, the final prosthetic restoration was completed, yielding an acceptable esthetic result (Fig. 9). Radiographic evaluation performed 6 months after the GBR and RPSCTG showed stable alveolar bone level (Fig. 10). The RPSCTGs were vitalized without any complications.
DISCUSSION
Hard and soft tissue augmentations prior to prosthetic treatment or implant therapy are required when the alveolar ridge has insufficient height and width. Various hard tissue augmentation procedures have been described to enhance the height and width of the alveolar ridge, including block bone grafts, particulate grafts, GBR, ridge expansion, and distraction osteogenesis [6,7,8,9,10,11,12]. After hard tissue grafting, the bone graft materials and barrier membrane should be completely covered throughout the healing period [21]. In particular, primary soft tissue closure seems mandatory for the success of the augmentation in GBR [7,22,23,24,25]. Several surgical techniques have been designed to acquire primary closure after the grafting procedure.
The classical buccal mucoperiosteal flap was originally described in the 1930s by Rehrmann [26]. Undermining of the buccal flaps and the periosteal incisions at their bases are required to achieve tension-free sutures. Subsequently, the buccal flap should be displaced coronally and sutured to cover the graft site completely [27]. The disadvantages of this flap advancement are the reduction of the vestibular sulcus depth and keratinized gingiva width [28]. Various techniques have been described to overcome these issues, including free autografts [13,14], a coronally positioned palatal sliding flap [16], palatal advanced flap, rotated palatal flap [16,17,18], and vascularized interposition periosteal connective tissue flap [29]. Augmentation can recreate the alveolar defects as a smooth and abundant alveolar ridge, thereby improving the esthetic appearance and providing for good prosthetic and gingival hygiene.
In our study, the double RPSCTG technique was used to cover the bone graft materials and barrier membranes. The advantages of this technique are that it provides sufficient soft tissue thickness, ample vascular supply, and protection of important anatomical structures such as the incisive neurovascular bundle and patatal donor tissue as well as patient comfort. The volume of soft tissue augmentation that can be performed simultaneously with bone grafting procedures is limited because of the requirement for flap closure and the compromised blood supply [30]. Compared to the free autograft, the pedicled flap is much more predictable and has a much better chance of survival over poorly vascularized areas such as the bone graft or nonresorbable membrane [18]. In this case, the pedicled flap receives its blood supply from the incisive vessels and its design is constructed to maintain a length-to-width proportion within 4:1 for adequate vascularity [29,31]. Additionally, a previous study showed that stabilizing the tissue with the pedicled flap is easier than stabilizing it with the free flap [18].
No signs of infection or suppuration were observed in the soft tissues of the donor and recipient sites during healing. The nonresorbable high-density polytetrafluoroethylene membrane appeared exposed at 4 weeks after stage 1 surgery. The membrane may have been exposed because the initial defect size was too large or the blood supply to that area was too low. Moreover, the fact that the patient smoked may have affected the recovery. No sign of infection was observed in the exposed site of the nonresorbable membrane. These findings are consistent with those of previous studies that described a favorable tissue response and biocompatibility at the barrier membrane. However, possible negative influences of early membrane exposure were reported in previous studies; therefore, additional soft tissue augmentation was used to cover the exposed bone graft materials, and the subepithelial connective tissue was harvested from the contralateral palate, similar to the technique used in stage 1.
The nonresorbable membrane was removed, and the contralateral RPSCTG was covered and sutured on the augmented site. The surgical site healed well with complete coverage by the end of the healing period. Several previous articles showed that early membrane exposure inhibited bone regeneration at the GBR sites [32,33,34,35]. Although primary coverage was not obtained at stage 1 in our case, acceptable outcomes were observed after the stage 2 surgery. The superficial epithelial flap was reflected and rotated posteriorly in the palatal site, and then the deep subepithelial flap was subsequently elevated and rotated anteriorly. Thus, the incisive neurovascular bundle could be protected avoiding full-thickness flap elevation. This technique prevents injury of the incisive neurovascular bundle. Furthermore, contraction may be minimized to a greater extent with the incisive vessel-based flap than with the free grafts [31]. Unlike the vascularized interposition periosteal connective tissue flap, the RPSCTG was made by two parallel incisions that improve the ability to harvest connective tissue. In addition, the distance of flap advancement in the RPSCTG may be elongated by using either rotation or rolling around the axis. Moreover, the palatal connective tissue graft may be useful in several other possible situations requiring periodontal surgery [14,36,37,38]. Many factors should be evaluated before palatal graft, such as the palatal vault anatomy, wound healing from the donor site, postoperative patient discomfort, the blood supply, and the need for sutures, stents, or hemostatic agents [39]. In addition, the amount of tissue required for harvesting can be mostly based on the thickness of the palatal tissue because graft success is closely correlated with the thickness of the palatal tissue. The limitations of harvesting palatal tissue are usually caused by an insufficient thickness of the soft tissue [38]. Therefore, bone sounding of the palatal masticatory mucosa is essential to determine the thickness of the soft tissue. The area between the maxillary first molar and canine may provide sufficient donor tissue while reducing the risk of disrupting the associated neurovascular structure. The most common postoperative complications associated with the palatal connective tissue graft procedure are prolonged bleeding from the palatal donor sites and patient discomfort [38]. Grafting from the deep subepithelial layer minimizes the amount of exposed palatal tissue by covering the superficial epithelial layer; consequently, the donor site is easily revitalized. Covering the superficial layer can decrease the exposed bone area and diminish the possibility of bleeding, thereby increasing patient comfort. This technique provides acceptable soft tissue architecture without diminishing the keratinized mucosa in the buccal aspect of the anterior maxilla. Moreover, this technique can satisfy both the patient's expectations and functional demands esthetically.
In conclusion, the RPSCTG technique may be useful for treating anterior maxillary defects by allowing for soft tissue coverage of the GBR site. To achieve favorable results, the surgeon should evaluate the anatomical structures, manage complications such as flap necrosis, and cooperate and communicate fully with the restorative dentist.










 XML Download
XML Download