

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Nearly 40% of the world's tobacco users live in just two countries, namely China and India [1]. Smoking is a risk factor for periodontal disease and is detrimental to oral health [2]. Increased alveolar bone loss, increased number of deep pockets, greater calculus formation, and poor response to periodontal therapy are some of the effects of smoking [2,3,4]. Evidence suggests that increased periodontal destruction is directly related to smoking, thereby influencing the host immune system and modifying the host response in the presence of plaque bacteria [3]. In contrast, smokeless tobacco products such as snuff, moist snuff, and chewable forms like gutka, zarda, khaini, mawa, and pan are most commonly associated with oral leukoplakia and oral submucous fibrosis [5], while periodontal effects include localized gingival recession (RC) and clinical attachment loss [6,7].
The practice of gutka chewing is common in communities particularly from South-East Asian countries including Bangladesh, Pakistan, Nepal, and Sri Lanka, and is spreading to North America [6,7,8]. In India, in the Global Adult Tobacco Survey, 21% of the participants were chewers of tobacco-related products [9] and the consumption of these products has resulted in the highest global oral cancer rate [10]. Gutka chewing is the most popular form of chewable tobacco used in India with the prevalence rate of as high as 57.6% [11]. Gutka is the generic name for a chewable form of smokeless tobacco that is a concoction of areca nut, powdered tobacco, slaked lime (aqueous calcium hydroxide), catechu, menthol, perfumery compounds such as sandalwood and musk ketones, and certain sweetening and flavoring agents [11]. Our literature search showed that there are relatively few reports on the harmful effects of gutka chewing on periodontal tissues and the findings of these studies reveal an increased prevalence of gingival RC as compared to periodontal pockets [12,13]. The biological plausibility of increased periodontal destruction in gutka chewers could be direct contact destruction by the influence of the gutka components on the periodontium or the host-mediated up-regulation of the systemic/local inflammatory status [13]. The effects of gutka chewing on the host immune response, mechanism of destruction, and progression of periodontal disease have not been clearly determined.
Periodontitis results in the destruction of tooth-supporting structures by releasing various host-mediated inflammatory mediators and tissue-destructive enzymes [2]. Two prominent inflammatory mediators, interleukin-1β (IL-1β) and IL-8 have been implicated in gingival and periodontal inflammation and assessing their levels might reveal the local status of the periodontium with respect to gutka chewing [14,15]. Chang et al. [16] and Jeng et al. [17] stated that areca nut and powdered tobacco, the two main ingredients of gutka, are independent risk factors for periodontal inflammation. A recent study showed that areca nut extracts increased the levels of IL-1β, IL-6, IL-8, and tumor necrosis factor-alpha (TNF-α), which are responsible for amplifying the inflammatory response in periodontal tissues [18,19]. IL-1β is an important cytokine that stimulates bone resorption and inhibits bone formation, thereby stimulating prostaglandin synthesis and protease production leading to the up-regulation of the inflammatory response [14]. IL-8 is a chemokine, which has chemotactic functions for polymorphonuclear leukocytes, lymphocytes, and macrophages, and this chemotactic effect is responsible for periodontal tissue destruction [15]. IL-1β and IL-8 production and secretion are increased when cells come in contact with nicotine [3,20]. Gingival keratinocytes, the first cells in contact with the chemicals of gutka, are the early producers of IL-1 and IL-8 and are responsible for the activation of the innate immune response to bacterial plaque and noxious agents [21]. Therefore, these are the potential mediators involved in gutka chewing-induced periodontal changes, and an assessment of these cytokines will characterize the impact of gutka and periodontitis on the host response. In addition, the areca nut, which contains arecoline and nicotine, inhibits the growth and attachment of fibroblasts, inhibits protein synthesis, suppresses the differentiation and functionality of dendritic cells, and might be cytotoxic for periodontal fibroblasts, leading to the progression of the pre-existing periodontal disease and impairment of the periodontal attachment [16,17].
There is abundant documentation of the adverse effects of smokeless tobacco on oral health, but there is a gap in knowledge regarding the effect of gutka chewing on the pathogenesis of periodontal disease. We hypothesized that gutka chewing may result in the up-regulation of proinflammatory mediators causing a further increase in the severity and progression of periodontal disease. To the best of our knowledge, there are no studies that have investigated the effects of gutka chewing on gingival inflammation by quantifying the proinflammatory cytokine levels. Gutka chewing and periodontitis are common findings among the rural population of India [22]. Therefore, the purpose of this study was to examine the effect of gutka chewing on periodontitis by evaluating the gingival crevicular fluid (GCF) levels of IL-1β and IL-8 and comparing them against those of nongutka chewers with periodontitis and of periodontally healthy controls.
MATERIALS AND METHODS
This cross-sectional study was conducted in Department of Periodontology, Chhattisgarh Dental College and Research Institute, Rajnandgaon, India, to evaluate the level of inflammatory markers among gutka chewers with periodontitis. The study was conducted from May to August 2013 after being approved by the Institutional Ethics Committee (CDEC/03/2013/03/GC). All the patients were from the rural population of Rajnandgaon district, India. Written informed consent was taken from all patients before inclusion in the study.
Sample size
The sample size was calculated using variations reported for the IL-1β levels in picograms per microliter by Tymkiw et al. [3]. The minimum expected difference between the two groups was assumed to be 100, and the assumed standard deviation was 90. Therefore, at an α error of 0.05 and power at 80%, the calculated sample size was 15 for each group.
Study population
A total of 45 subjects in the age range of 18-60 years were enrolled in this study. Fifteen periodontally healthy subjects as controls (group I, HC) and 30 patients with periodontitis (15 gutka chewers [group II, GCP] and 15 nongutka chewers [group III, NGC]) were selected. The Centers for Disease Control and Prevention (CDC) Periodontal Disease Surveillance Workgroup and American Academy of Periodontology (AAP) definition for moderate periodontitis was adopted in our study. Periodontitis was diagnosed when ≥2 interproximal sites with a clinical attachment level (CAL) of ≥4 mm (not on the same tooth) or ≥2 interproximal sites with probing depth (PD) of ≥5 mm (not on the same tooth) were present [23]. Healthy subjects were nontobacco users who presented with no sites of attachment loss or PD ≥4 mm. Gutka chewers with periodontitis were enrolled if they were chewing currently at least one sachet of gutka daily for at least the past year [24]. A sachet of gutka in common usage contains 1.5 g of the processed product. Periodontitis patients who reported to have never consumed tobacco in any form were categorized as nongutka chewers.
The following were the enrolment criteria for all subjects: dentate with at least 20 teeth; good general health; nonsmoker; and no corticosteroid, antibiotic, and/or nonsteroidal anti-inflammatory medication usage within 6 months. The exclusion criteria were as follows: alcohol consumption; current or former user of other tobacco products; pregnant and lactating mothers; and patients who underwent scaling and root planing in the last 6 months.
A detailed interview of the selected individuals was conducted regarding age, sex, gutka usage (yes/no), duration of gutka consumption, and duration of placement of gutka in the mouth by a trained interviewer (R.P.P.). This was followed by a periodontal examination by an examiner (S.N.) and the collection of GCF by another examiner (P.S.J).
Clinical parameters
The full-mouth plaque index (PI) [25], gingival index (GI) [26], PD, CAL, and RC were recorded for all the groups. All recordings were taken from six sites (mesio-buccal, midbuccal, disto-buccal, disto-lingual/palatal, midlingual/palatal, and mesio-lingual/palatal). PD, CAL, and RC were measured to the nearest millimeter with a straight periodontal probe (UNC-15, Hu Friedy, Chicago, IL, USA). PD was defined as the distance from the coronal-most margin of the free gingiva to the most apical penetration by a probe. CAL was defined as the distance from the cemento-enamel junction (CEJ) to the most apical penetration of the probe, and RC was measured from the CEJ to the gingival margin.
Examiner calibration
All the measurements were performed by one trained and calibrated periodontist (S.N.). As a part of the calibration process, 20 sites were examined twice, 24 hours apart before the start of the study. Calibration was accepted if measurements at baseline and 24 hours were similar to 1 mm at the 95% level (correlation coefficients between duplicate measurements; r=0.95). The examiner was blinded to the patient's group and interview recordings.
GCF sample collection and assessment
In the periodontitis group, GCF collection was done from five nonadjacent sites with the greatest PD selected at least 1 day after clinical examination. The selected sites for sampling were air-dried and isolated with a roll of cotton, and the supragingival plaque was removed without touching the marginal gingiva. Samples of GCF were obtained by placing a white color-coded 1- to 5-µL calibrated volumetric microcapillary pipette (Sigma Aldrich Chemical Co., St. Louis, MO, USA) on the site. A pooled GCF of 3 µL was collected by keeping the micropipettes at five sites, for not more than 5 minutes at each site, and the pooled volume was calculated. The sites from which no GCF could be obtained or at which the micropipette was contaminated with blood and saliva were discarded and excluded from the study. The GCF collected was immediately transferred into a plastic vial and frozen at -70℃ until the time of assay.
IL-1β and IL-8 analysis in GCF
A quantitative sandwich enzyme-linked immunosorbent assay (ELISA) (Quantikine, R&D Systems, Minneapolis, MN, USA) specific for human IL-1β and IL-8 was used to measure the IL-1β and IL-8 levels in the pooled GCF samples. The procedure was carried out according to the manufacturer's instructions. Each sample was assayed in duplicate standards and controls; high, medium, and low were included in each run. All results were reported within the linearity of the assay. The colorimetric reactions were read as the value of the optical density directly on the automatic microplate reader set to 450 nm. The concentrations of IL-1β and IL-8 were reported in picograms per microliter (pg/µL) of the sample. All GCF sampling and ELISA assays were performed by one examiner (S.J.P.) blinded to the clinical results.
Statistical analysis
Data were entered and analyzed using the SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA). Normality of data was analyzed, and a nonparametric approach was used on the basis of the data distribution. For GI and PI, one-way analysis of variance (ANOVA) followed by post hoc Tukey test was done for comparison among the GCP, NGC, and HC groups. The IL-1β and IL-8 levels were analyzed by the Kruskal-Wallis ANOVA test for comparison among the three groups and the Mann Whitney test for comparing two groups. A parametric unpaired t-test was conducted for PD, RC, and CAL among the two periodontitis groups. To evaluate the correlation between the duration of gutka chewing and RC, CAL, PD, IL-1β, and IL-8, Pearson's correlation coefficient was calculated. In each case, the level of significance was set at P<0.05. The power of the present study was 83%.
RESULTS
Subject characteristics (Table 1)
In all, 45 patients were examined for this study, with 15 participants in each group. The mean age of the GCP group was 40.8±14.1 years; the NGC group, 42.9±11.6 years; and the HC group, 28.3±6.4 years. There were two females in the GCP group, four in the NGC group, and five females among the healthy patients. The average duration of gutka chewing was 11.3±9.6 years, and the duration of gutka placement in the mouth was 32.6±7.9 minutes.
Clinical parameters (Table 2)
The PI and GI values showed significant differences when compared group-wise (P<0.001), but this difference was only present when healthy subjects were compared to the periodontitis groups; no significant difference was seen between the two periodontitis groups. PD was significantly more for the NGC group (3.18±0.52, P=0.002) than for the GCP group (2.64±0.28). In contrast, RC and the CAL were higher for the GCP group (2.02±0.31, 4.60±0.56) than for the NGC group (1.21±1.15, 3.70±0.32), and the difference was of statistical significance (P=0.013, P<0.001).
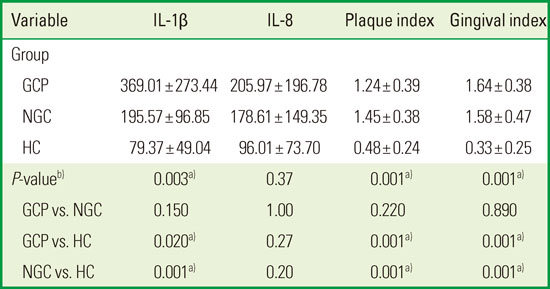
Cytokine levels (Tables 3 and 4)
When compared group-wise there was a statistical significance for IL-1β (P=0.003) and no difference for IL-8 (P=0.37). There was an increase in the IL-1β and IL-8 levels among the GCP subjects (IL-1β, 369.01±273.44 pg/µL; IL-8, 205.97±196.78 pg/µL) as compared to the NGC subjects (IL-1β, 195.57±96.85 pg/µL; IL-8, 178.61±149.35 pg/µL) although it was not significant (P=0.15, P=1.00). When the HC group was compared against the GCP and the NGC groups, a significant difference was seen only for IL-1β (P=0.020, P=0.001) and not for IL-8 (P=0.27, P=0.20). Therefore, the IL-1β levels increased significantly for the periodontitis group as compared to the HC group, and no significant increase was observed when the GCP and the NGC groups were compared, whereas the IL-8 levels showed nonsignificant changes in all the comparisons. A correlation analysis revealed that the duration of gutka chewing was correlated to the IL-8 levels only.
DISCUSSION
The present study was conducted to explore the role of gutka chewing on the pathogenesis of periodontitis by assessing the levels of inflammatory mediators. To the best of our knowledge, the present study represents the first report on the effect of gutka on the periodontal health of the rural population of Rajnandgaon and gutka chewers. Pan, gutka, pan masala, pan mawa, zarda, and khaini are some of the popular tobacco and areca nut combinations in India [11]. Gutka is the most popular commercial preparation of areca nut and tobacco [22,24]; it is a powdery, granular, light brownish to whitish substance. It is placed between the teeth and the buccal mucosa and is gently chewed or sucked over a period of time after which it is either spat out or swallowed [11,22,24]. Even though gutka chewing is banned in Rajnandgaon, it is still distributed and consumed illegally by many people [27]. Our study had male and female patients who were gutka chewers for more than 10 years. Similar reports were published by Joshi et al. [11]. Women prefer smokeless tobacco due to the social disapproval of smoking, which makes them more vulnerable to gutka addiction. There is a significant difference between the age group of the control group and that of the other groups. This implies that the age group is determined by the prevalence of periodontitis. A similar aged control group would have given a more reliable conclusion as at least a few members of the selected group in our study could be susceptible to future periodontitis.
The periodontitis case definition used in our study was given by CDC-AAP [23]. This definition uses both the PD and CAL, and has been considered a standard in the field [28]. The definition is very specific as it includes the attachment loss in the interproximal surfaces as the criteria for defining periodontitis. This helped us exclude subjects who had periodontal loss due to reasons other than periodontitis, including gutka chewing [28]. The results of our study reveal that gutka chewers with periodontitis had more gingival RC than nonchewers with periodontitis. The RC observed was not site-specific to the area of placement but was observed on the whole mouth. RC occurs as a result of the apical proliferation of the epithelial attachment and connective tissue destruction, which may be related to the local irritating effects of gutka, as well as host or bacterial factors [13]. In our study, RC might have occurred due to the mechanical and/or chemical trauma to the gingiva from the components of gutka, resulting in increased periodontal destruction. Gutka contains fine grains of areca nuts, which may cause mechanical injury, and allows the ground tobacco to adhere to the traumatized mucosa, leading to morphological changes and tissue damage [29]. These findings are in agreement with those of previous studies by Singh et al. [30] and Parmar et al. [22] in India. Various authors have reported that buccal sites usually exhibit a thin alveolar bone causing alveolar dehiscence, and that tobacco chewing is likely to cause chemical injury to the thin gingiva, leading to the loss of marginal gingiva [31]. Like RC, the CAL was significantly higher in gutka chewers. Gutka in our sample was not placed at specific areas of mouth as in the case of other smokeless forms of tobacco [6,7]. This could be the reason for the generalized gingival RC, and hence, loss of attachment, as compared to that in specific areas, which also necessitated full-mouth probing parameters. Attachment loss is an important component of the periodontal disease measure that defines the past history of the disease. Periodontal destruction was enhanced as the CAL increase was not only due to the conversion of pockets to RC sites but also due to the consumption of gutka. Dehlen et al. [32] showed similar findings; however, a few studies have shown conflicting results [22,24,29,33]. Hence, there is a possibility that the local effect of gutka can enhance the local progression of periodontitis.
In our study, gutka chewers had higher plaque and gingival inflammation than healthy patients; these findings are consistent with those of studies by Chu et al. [6], Singh et al. [30], and Javed et al. [29,33], but in contrast to the findings of Robertson et al. [7] and Dahlen et al. [32]. Poore et al. [34] revealed site-specific gingival inflammation at the area of placement. However, among the periodontitis group, when gutka chewers were compared with the nonchewers, there was no difference in plaque levels and gingival inflammation. A direct comparison was not possible due to a lack of studies among gutka chewers. David et al. [35] showed that gutka chewing was a protective factor for calculus formation and may have both in vitro and in vivo antimicrobial effects, which could be the reason for the insignificant changes in plaque. It has been suggested that a betel stain often coats the teeth, which may act as protective varnish [35].
The GCF volume increases with periodontal inflammation, its flow rate increasing up to 30-fold in periodontitis sites as compared to healthy sites [3,14,15]. The collection of GCF was relatively noninvasive, making GCF a convenient tool to evaluate the markers of periodontal inflammation [15]. We used micropipettes to collect GCF in a manner similar to the method used by Faizuddin et al. [14]. The magnitude of inflammation can be determined by measuring proinflammatory and immuno-regulatory cytokines and chemokines in the GCF. In our study, we wanted to study the effects of gutka chewing on periodontal inflammation, and IL-1β and IL-8 are considered as suitable candidate molecules for monitoring the progression of periodontal disease [14,15].
Areca nut is the endosperm of the fruit of the areca catechu tree. The pharmacological effects of areca nut include addiction, euphoria, excessive salivation, and tremors, attributed to arecholine, the major alkaloid in areca nut [18]. The alkaloid arecholine regulates the inflammatory process by eliciting prostaglandin E2 (PGE2), IL-1β, IL-β, IL-6, and TNF-α [18,19] and causes the depression of antioxidants such as superoxide dismutase, catalase, and glutathione-S-transferase, leading to oxidative stress [29]. They are cytotoxic for oral epithelial cells and fibroblasts and can inhibit cell migration, spreading, growth, and collagen synthesis, making them more susceptible for periodontal damage [16,17,29]. Nicotine is the other major constituent in gutka, which can directly modify the production of cytokines and inflammatory mediators, causing increased PGE2, IL-1β, IL-1β, and IL-8 production by gingival keratinocytes [21]. Nicotine has a deleterious effect on the gingival and periodontal fibroblasts. Arecoline and nicotine are known to have a synergistic effect, leading to further periodontal breakdown. Slaked lime causes an increased cell turnover rate, increased production of reactive oxygen species, DNA damage, and chromosomal abnormalities [29]. We hypothesized that there could be a rise in the proinflammatory cytokine by the introduction of these chemicals into the blood stream through the diseased periodontium, aggravating the host response, but our study failed to show such a response.
In our study, the IL-1β and IL-8 GCF levels were elevated in gutka chewers but did not reach statistical significance when compared with the nonchewing periodontitis subjects. The physical placement of gutka on the external tissue surface did not affect the GCF cytokine levels and the increased levels of interleukins are more likely due to periodontal disease. As this was the first study assessing the levels of cytokine among gutka chewers with periodontitis, a direct comparison with other research was not possible. However, tobacco smokers with periodontitis showed an increase in IL-1β [3] and IL-8 [36] in the GCF levels as compared to nonsmokers with periodontitis. All research has focused on the comparison of chewers with periodontitis against healthy subjects. In our study, gutka chewers with periodontitis had higher IL-1β levels than the healthy subjects. Similar findings were obtained in in vitro studies from smokeless tobacco users [37] and those using cigarette smoke extract [38]. Poore et al. [34] showed no alternation in IL-1β secretion after nicotine application on lipopolysaccharide treated human monocytes. When nicotine was applied in vitro on peripheral blood monocytes and lymphocytes and on gingival mononuclear cells of patients with periodontitis, no effect on IL-1β was seen. The authors suggested that nicotine cannot activate more due to the maximal previous stimulation by periodontal disease [34]. Arimilli et al. [38] reported that cigarette smoke extract inhibited the secretion of IL-1β. This cytokine resulted in T cell and NK cell anergy causing impairment of the ability to fight viral and bacterial infection [38]. The nonchewer periodontitis groups in our study had significantly higher IL-1β levels than the healthy group. This is consistent with other studies showing higher GCF IL-1β levels in patients with aggressive or chronic periodontitis as compared to healthy controls [3,36]. Gutka chewing per se has a limited effect on the pathogenesis of periodontitis. Our study had a relatively high nonhomogeneity in the GCP subjects with respect to the duration of their habit. This variation could probably have confounded the role of this form of tobacco in the pathogenesis of periodontitis. Studies with a larger sample of GCP are required to establish this relationship.
Our study did not find any difference in the IL-8 levels when the periodontitis groups were compared with the group of healthy subjects. IL-8 is a multifunctional cytokine that plays a role in immune and inflammatory activities like the recruitment and activation of neutrophils. A review of IL-8 showed that its level is not consistently raised in all periodontitis subjects [39]. The population of periodontitis subjects in our study did have raised IL-8 levels, which were, further, not affected by gutka chewing. It has been found that nicotine has a suppressive effect on the innate response to infection by reducing the activity of antimicrobial peptide [4]. Arimilli et al. [38] found that smokeless tobacco extract and nicotine decreased IL-8 levels secreted by mononuclear immune cells. Kamma et al. [40] also showed no effect among smokers, and Tymkiw et al. [3] showed a decrease in this chemokine response among smokers with periodontitis. As the GCP group had more variation in the duration of gutka chewing, we wanted to see if this aspect was correlated with the clinical parameter and interleukin levels. Only IL-8 was negatively correlated. This intriguing influence of periodontitis and smokeless tobacco on IL-8 warrants further exploration as we could not reach a conclusion on the basis of these findings.
There were a few limitations of our study. The cross-sectional nature of the study design does not tell us the temporal direction of the relationship between gutka chewing and periodontitis. A larger sample would have helped us to achieve a more homogenous GCP population with respect to the duration of the habit. Further, the healthy controls were younger than the subjects in the diseased groups. Within the limitation of the study, it can be concluded that gutka chewing did not have any effect on the IL-1β and IL-8 levels in GCF. Gutka chewing was associated with localized enhanced periodontal destruction, which can be attributed more to the chemical and irritant effects of gutka chewing than to any influence on periodontitis pathogenesis. Our study concurs with other research showing that there is an increase in periodontal destruction among gutka chewers reflected in the attachment loss than compared to the actual periodontal pocketing. Further studies are required for assessing the qualities of periodontal cells affected by gutka chewing, and further information on the expression of the other cytokines will clarify the effects of gutka chewing on periodontitis.


 XML Download
XML Download