

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Implant stability at the time of surgery is crucial for the long-term success of dental implants. Primary stability is considered of paramount importance to achieve osteointegration [1]. Primary implant stability can be defined as a function of local bone quality and quantity, the geometry of an implant, the placement and surgical technique used, and the precise fit in the bone. Thus, primary implant stability is considered a significant parameter in achieving osseointegration, and the orchestration of the elements mentioned is crucial for the long-term success of the implant [2,3].
Two main factors that influence primary stability of an implant during placement are the amount of bone-implant contact and the role of compressive stresses at the implant-tissue interface. Such stresses may be beneficial for enhancing the primary stability of an implant, but they can reach a sufficiently high level to result in necrosis and local ischemia of the bone at the implant-tissue interface [4-6]. In the same respect, secondary stability can also be determined by the bone tissue response to the surgical trauma and the implant surface. The response is ultimately bone formation and remodeling at the implant interface leading to increased fixation and stability of the implant, although bone resorption resulting in implant failure can also occur during the initial healing period. In the literature, it is clear that surface roughness may result in more bone at the implant interface as well as a higher resistance to torque. Poor fixation may lead to micromovements during implant healing, which can potentially cause fibrous encapsulation and are associated with higher failure rates. Shorter healing periods are usually needed for implants with good primary stability. On the other hand, implants with poor stability need longer healing periods to achieve sufficient gain in secondary stability. This suggests the possibility of determining the length of the healing period on an individual basis, making implant treatment safer, more effective, and less time-consuming in some cases [7].
Generally, clinicians evaluate primary stability using the percussion test or using their own perception during the insertion process. However, the lack of precision has motivated the development of different methods to objectively evaluate primary stability; in particular, peak insertion torque (IT) and resonance frequency analysis (RFA) are the most used globally. Clinically, RFA values or implant stability quotient (ISQ) values have been correlated with changes in implant stability during osseous healing. Thus, IT and ISQ values are thought to have a positive correlation [8,9]. However, the formula of higher IT torque translating into higher primary stability may not always be true because the quantity and quality of bone varies significantly among patients. Therefore, the purpose of the present study was to investigate the correlation between IT and primary stability of dental implants using artificial bone blocks with different bone densities and compositions to mimic different circumstances that are encountered in routine daily clinical settings.
MATERIALS AND METHODS
Bone specimens
The bone block of solid rigid polyurethane foam (Sawbones, Vashon, WA, USA) with various bone densities (cancellous bone: #10, #20, #30; cortical bone: #50; and homogeneous bone: #10, #20, #30, #40) were used in the present study (Fig. 1). Because the mean bone mineral density was 0.31 g/cm3 for the posterior maxilla and 0.55 g/cm3 for the anterior maxilla, polyurethane foam blocks with a bone density of 0.48 g/cm3 were chosen. Short fiber-filled epoxy sheets were used as a substitute for cortical bone. Because the mean cortical thickness for the mandible was 2.22±0.47 mm and the mean cortical bone thickness for the maxilla was 1.49±0.34 mm, the sheets with a corresponding thickness were selected [10]. The following five different cortical thicknesses were used: blocks without a cortical layer (only homogeneous bone), blocks with a 0.5 mm cortical thickness, blocks with a 1.0 mm cortical thickness, blocks with a 1.5 mm cortical thickness, and blocks with a 2.0 mm cortical thickness.
Experimental design
The experimental group under evaluation was subdivided into 5 subgroups according to the objectives. In group 1, the correlation between IT and implant stability according to the bone density was evaluated. Implants were placed in homogeneous bone blocks with different bone densities (#10, #20, #30, and #40) following osteotomy preparation with a final drill diameter of Ø3.6 mm. An increase in numerical size of the bone blocks represented an increase in the bone density. Measurement of the IT and ISQ values were repeated 20 times for each bone density. In group 2, the correlation between the IT and implant stability according to the size of the final drill diameter used was evaluated. Homogeneous bone blocks with a density of #20 were used.
The final drill diameters under evaluation were Ø2.7 mm, Ø3.0 mm, Ø3.3 mm, and Ø3.6 mm. The remaining process was identical to that for group 1. The objective of group 3 was to evaluate the correlation between the IT and implant stability according to the thickness of the cortical bone. Using bone blocks with a cortical density of #50 and cancellous density of #20, the cortical bone was manipulated to have a thickness of 0.5 mm, 1.0 mm, 1.5 mm and 2.0 mm. Again, the final drill diameter was Ø3.6 mm and identical steps were performed.
The objective of group 4 was to evaluate the correlation between the IT and implant stability according to the cancellous bone density by controlling the cortical bone thickness to 1.5 mm and using block bones with a uniform cortical density of #50. Only the density of the cancellous bone (#10, #20, and #30) was different in the bone blocks for group 4.
In group 5, the correlation between the IT and implant stability according to the size of the final drill diameter in the bone blocks with a uniform cortical thickness of 1.5 mm was evaluated. The density of the cortical bone (#50) and the cancellous bone (#20) was controlled. The final drill diameters were Ø3.0 mm, Ø3.3 mm, Ø3.6 mm, and Ø3.8 mm.
Osteotomy preparation and fixture installation
All of the osteotomies were prepared with a gentle surgical technique using a surgical drill at a rotational speed of 800 rpm with opious external cooling. The drill was fixed in a standard drilling set equipped for constant drilling. After drilling, the implant fixtures (Osstem Implant Co., Seoul, Korea) with a length of 11.5 mm and a diameter of 4.1 mm were placed in the prepared osteotomies. The diameter of the final drill was chosen and assigned according to the test protocol. The following diameters were used: Ø2.7 mm, Ø3.0 mm, Ø3.3 mm, Ø3.6 mm, and Ø3.8 mm (Fig. 2).
IT and RF measurements
During installation, the peak IT was measured for all of the implants (Fig. 3). Following the final seating of the fixtures, the stability of each implant was measured in ISQ units using the Osstell Mentor (Osstell, Göteborg, Sweden). The RF values were represented in the ISQ on a scale from 1 to 100 and were averaged for each implant (Fig. 4). Each measurement was performed up to 20 times [11-15].
Statistical analysis
The IT and ISQ values were summarized using means and standard deviations. One-way analysis of variance was used to compare the mean IT and ISQ values. The Pearson's correlation coefficient was used to evaluate the correlation between the IT and the ISQ at implant placement. A P-value of <0.05 was considered statistically significant. Statistical analysis was performed using the IBM SPSS ver. 20.0 (IBM Co., Armonk, NY, USA) [16-22].
RESULTS
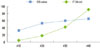
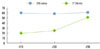
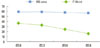
In group 1, the mean IT and ISQ value increased as the density of bone blocks increased, respectively (P=0.00 and P=0.00). The correlation between the two parameters was evaluated using Pearson's correlation coefficient, and the results suggested a positive correlation (CQ=0.82, P=0.00), which was statistically significant (Table 1, Fig. 5). For group 2, the mean IT values decreased as the final drill size expanded, but this was not the case for the ISQ values. The mean ISQ values showed limited change as the drill size increased. The correlation coefficient between the IT and ISQ value was -0.07 with a P-value of 0.77, but it was considered non-significant (Table 2, Fig. 6). The mean IT values in group 3 increased according to the thickness of the cortical bone, and the same was true for the ISQ values as well. It was also shown that the two parameters had a stronger linear relationship (CQ=0.84) with the values reaching statistical significance (P=0.00) (Table 3, Fig. 7). For group 4, the mean IT values increased as the cancellous bone density increased (P=0.00), but the correlation with the ISQ values was weak (CQ=0.45) and nonsignificant (P=0.09) (Table 4, Fig. 8). Finally, in group 5 the mean IT decreased according to the final drill size (P=0.00), but the correlation with the ISQ value was weak (CQ=0.57) and was non-significant (Table 5, Fig. 9).
DISCUSSION
The aim of the present study was to investigate the correlation between the IT and primary stability of dental implants through the IT test, and RFA analysis was performed using artificial bone blocks that simulated different circumstances that can ioccur in clinical practice. In general, primary implant stability is considered the most important factor in a successful implant treatment, and the distinct ranges of implant primary stability have been distinguished by the resonance frequency method [23-27]. Thus, RFA was used instead of the Periotest as a method to measure implant stability.
The results of the present study showed that the IT and initial stability increased according to the increase in the bone density, resulting in a strong positive correlation. In other words, the initial stability was shown to be highly dependent on the bone density. The IT also increased according to the thickness of the cortical bone, and a slight increase was observed for initial stability. This shows that the volume of high dense cortical bone affects the initial stability and it corroborates a recent study in which the same artificial bone model was used. In that study, an increase in the mean IT values was observed when the bone blocks with only trabecular bone (without a cortical layer) were compared to the groups with a cortical layer of 1 mm, 1 to 2 mm, and 2.5 mm [10].
The results from group 4 did not deviate much from group 2, which may suggest that the density of cancellous bone may have an impact on IT, but may have a limited effect on primary stability. This may indicate that the thickness of cortical bone or the cortical outer layer functions as the primary determinant for primary stability. This was also reflected in the results of groups 2, 4, and 5, where the correlation between the two parameters was weak. Therefore, the only factors that showed a positive correlation between the IT and the ISQ value were the bone density and thickness of the cortical bone.
In testing the impact of the final drill size, the IT decreased as the drill size expanded, but the initial stability showed limited change. This showed that initial stability cannot be acquired by simply reducing the diameter of the final drill in attempts to increase the IT. Biologic and anatomical consequences such as the thickness of cortical bone seem to be significant factors affecting primary stability, and estimation of bone density and the optimal selection of drill size are important.










 XML Download
XML Download