

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In recent years, it has become clear that each person has a different gingival character. To describe this varying gingival architecture, including the thickness and width of labial gingiva, the term "periodontal biotype" or "gingival biotype" has been proposed [1]. There are two major gingival biotypes. The thin scalloped biotype represents high scalloped gingiva and osseous contour, narrow keratinized gingiva, and a triangular tooth form. The thick flat biotype shows flat gingiva and osseous contour, wide keratinized gingiva, and a square tooth form. Some gingival features are influenced by tooth shape, position, and size, as well as gender and age; in fact, it has been reported that many features of the gingiva are genetically determined [2,3].
Scaling and root planing (SRP) has been used in periodontal therapy. It includes the removal of plaque and calculus through repetitive instrumentation on the root surface. The main purpose of SRP is the reduction of the periodontal pocket. A periodontal pocket develops when the periodontium is destroyed by bacteria and exists as a reservoir of bacteria until it is eliminated by periodontal therapy such as SRP. This is achieved by not only the removal of bacteria but also the shrinkage of the gingiva that occurs during the periodontal healing period. It has been clearly established that shrinkage after SRP is inevitable.
Identifying each gingival biotype is important because they present different healing tendencies. Many studies have shown different outcomes after periodontal therapy according to gingival biotype. A greater regaining of soft tissue occurred in patients with a thick flat biotype following a crown lengthening procedure (CLP) than in patients with a thin scalloped biotype [4]. A higher prevalence of gingival shrinkage (GSH) was reported with a thin scalloped biotype, and this result was further supported by a study demonstrating an increased susceptibility to shrinkage in individuals with a thin, scalloped gingival architecture [5,6]. A thick flat biotype showed a greater prevalence of the presence of a papilla between an immediate implant and the natural teeth than did a thin scalloped biotype [7]. Also, thin gingiva was associated with poor outcomes of soft tissue regenerative surgery [8]. Identifying the gingival biotype by using reliable methods will allow the clinician to predict prognosis and avoid unexpected complications.
The therapeutic results of most periodontal therapy are influenced by gingival biotype, as mentioned previously. It is generally accepted that the dimensions of the gingiva in both the facial and interproximal areas shrink following SRP [9-12]. Although GSH after SRP is a common complication in periodontal patients, and several measurement methods, such as transgingival probing, probe transparency, visual inspection, and ultrasonic devices, have been used to determine gingival thickness [13], few studies on gingival biotypes have focused on alterations of the gingiva after SRP using an atraumatic method to examine the gingival thickness.
The present study was designed to examine the influence of gingival biotypes on the results of SRP using cone-beam computed tomography (CBCT), which is a less traumatic, and more precise and quantitative method of evaluating the gingival thickness.
MATERIALS AND METHODS
Study population
The present study included clinical data of 25 patients (17 males, 8 females) who visited the Department of Periodontology of Wonkwang University Dental Hospital. Patients diagnosed with chronic periodontitis were included. None of these patients had previously received periodontal therapy. The exclusion criteria were as follows: (1) prosthodontic crown, (2) pregnant or lactating female, (3) crowding which did not present an ideal arch on the maxillary anterior teeth, (4) medication with any known effect on gingival hyperplasia, (5) GSH over the mucogingival junction, or (6) a deep periodontal pocket depth (PPD) of over 7 mm.
The Institutional Review Board of Wonkwang University Dental Hospital approved the protocol (WKDIRB 201208-01). All of the subjects signed an informed consent document prior to engagement in the study.
Therapy
All of the patients were provided with full mouth scaling and oral hygiene instruction. By accurate and repetitive instructions on the roll brushing technique for patients, we could expect a similar outcome to that from the Bass and Stillman technique. Moreover, the roll technique is a more conservative method than the Bass and Stillman technique, which can cause unintended trauma to the gingiva [14]. Complementary instruments such as an interdental brush and dental floss were also recommended. Root planing was performed on the upper anterior teeth (upper right canine to upper left canine) at 2 weeks after scaling (baseline).
Clinical parameters
The periodontal parameters including the PPD and GSH were assessed and clinical photographs were taken at baseline and 3 months after SRP. All of the patients were treated by the same examiner.
1) Gingival thickness (GT) was evaluated using CBCT (Alphard-3030, Asahi Roentgen Co., Kyoto, Japan) in D mode (51×51 mm, voxel size 0.1 mm) at baseline (Figs. 1 and 2). Then, the GT at the sagittal midpoint of each of the central incisors was determined at 2 mm apical from the gingival margin. A 1.5-mm GT was considered the threshold distinguishing the thick biotype and thin biotype, in line with previous research [15]. To determine the GT in the maxillary anterior region, cotton rolls were used during radiation to separate the lip from the gingiva.
2) The PPD was measured to the nearest 0.5 mm at the labial side of the maxillary anterior teeth using a periodontal probe (Thin Williams Probe, Hu-Friedy, Chicago, IL, USA). The PPD was measured at baseline to avoid uncertain measurement caused by gingival swelling that could have been influenced by supragingival plaque and calculus.
3) GSH was also measured at baseline and 3 months after SRP. At baseline, the examiner had taken photographs of the maxillary anterior teeth in consistent condition (magnification 1:2, diaphragm 32, shutter speed 1/160 second) with a reference instrument as the periodontal probe. Photographs of same patient at baseline and 3 months after SRP were adjusted with each other on the monitor; then the GSH was assessed by using the image tool (Adobe Photoshop 7.0, Adobe Systems Inc., San Jose, CA, USA) at three points: (1) mesial papilla, (2) midfacial gingiva, and (3) distal papilla. All of the measurement points were evaluated using a constant landmark such as the incisal edge and end of the cusp to reduce distortion of the photographs and represented as the clinical crown length. The GSH were calculated by subtracting the values of the clinical crown length at baseline and 3 months after SRP (Fig. 3).
Group design
The maxillary anterior teeth including the incisors and canines were used in the present study. Three sites (mesial, middle, distal) at the labial side on each tooth were measured and divided into 4 groups as follows: (1) Shallow pocket and thin biotype (GS-n); the mean PPD extends 3-5 mm and the GT is thin, (2) shallow pocket and thick biotype (GS-k); the mean PPD extends 3-5 mm and the GT is thick, (3) deep pocket and thin biotype (GD-n); the mean PPD extends 5-7 mm and the GT is thin, (4) deep pocket and thick biotype (GD-k); the mean PPD extends 5-7 mm and the GT is thick. In analyzing the GSH, two more groups were considered as follows: (5) normal gingival crevice and thin biotype (GN-n); the PPD remains under 3 mm and the GT is thin. (6) Normal gingival crevice and thick biotype (GN-k); the PPD remains under 3 mm and GT is thick. In addition, interdental sites including mesial and distal sites and middle sites were divided to evaluate an effect of gingival biotype according to position of gingiva. All comparison were performed between baseline and 3 months after SRP.
Statistical analysis
The results of the therapy were compared to present the differences in the PPD and GSH between baseline and 3 months after SRP according to the gingival biotype using an independent t-test. All of the values recorded in the present study are presented as mean±standard deviation. IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA) was used for all statistical calculations. If any values did not satisfy normality in the independent t-test, the Mann-Whitney U test was performed.
Before this study, a power analysis with G*Power 3.1.3 (Franz Faul, Christian-Albrechts-Universität, Kiel, Germany) was performed to estimate the sample size. The sample size for the study of PPD was calculated based on a significance level of 0.05 and a power of 90%. The power analysis showed that 172 samples were required. The sample size for the study of GSH was calculated based on a significance level of 0.05 and a power of 95% requiring 210 samples. In this study, each sample size for PPD and GSH were 188 and 273, presenting enough sample size to fulfill requirement of power analysis.
RESULTS
The study population consisted of 25 patients suffering from periodontitis in the maxillary anterior area. During the experimental period, nine people were lost because of refusal of follow-up, or migration to another city. A total of 16 patients (9 males and 7 females; mean age, 49.31±7.90 years) consequently participated in the present study. Six patients presented thick gingiva while ten patients presented thin gingiva.
Changes in the PPD
Changes in the PPD according to gingival biotype
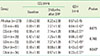
The PPD and PPD reduction are presented at Table 1. In GS-n, the PPDs at baseline and 3 months after SRP were 3.20±0.40 mm and 2.40±0.56 mm, respectively, and the PPD reduction was 0.80±0.61 mm. In GS-k, the PPDs at baseline and 3 months after SRP were 3.22±0.42 mm and 2.32±0.47 mm, respectively, and the PPD reduction was 0.90±0.61 mm. There were no significant differences between the two groups.
In GD-n, the PPDs at baseline and 3 months after SRP were 5.48±0.83 mm and 2.90±1.05 mm, respectively, and the PPD reduction was 2.59±1.05 mm. In GD-k, the PPDs at baseline and 3 months after SRP were 6.18±0.91 mm and 3.05±0.80 mm, respectively, and the PPD reduction was 3.14±0.64 mm. The PPD reduction showed a significant difference (P<0.05), but the PPD at 3 months after SRP failed to show a significant difference.
Changes in the PPD at the interdental and middle sites
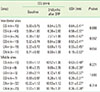
For more detailed information, all of the sites were classified into interdental sites (n=154) and middle sites (n=34) to evaluate the PPD separately by site (Table 2).
Interdental sites
In GS-n, the PPDs at baseline and 3 months after SRP were 3.21±0.41 mm and 2.46±0.58 mm, respectively, and the PPD reduction was 0.76±0.64 mm. In GS-k, the PPDs at baseline and 3 months after SRP were 3.23±0.42 mm and 2.34±0.48 mm, respectively, and the PPD reduction was 0.89±0.62 mm. There were no significant differences between the two groups.
In GD-n, the PPDs at baseline and 3 months after SRP were 5.42±0.78 mm and 2.96±1.00 mm, respectively, and the PPD reduction was 2.46±1.02 mm. In GD-k, the PPD at baseline and 3 months after SRP were 6.40±0.91 mm and 3.33±0.72 mm, respectively, and the PPD reduction was 3.07±0.70 mm. The PPD reduction showed significant differences between the two groups (P<0.05). However, the PPD at 3 months after SRP showed no significant difference.
Middle sites
In GS-n, the PPDs at baseline and 3 months after SRP were 3.13±0.34 mm and 2.13±0.34 mm, respectively, and the PPD reduction was 1.00±0.37 mm. In GS-k, the PPDs at baseline and 3 months after SRP were 3.17±0.41 mm and 2.17±0.41 mm, respectively, and the PPD reduction was 1.00±0.63 mm. There were no significant differences between the two groups.
In GD-n, the PPDs at baseline and 3 months after SRP were 5.80±1.01 mm and 2.60±1.34 mm, respectively, and the PPD reduction was 3.20±1.10 mm. In GD-k, the PPDs at baseline and 3 months after SRP were 5.72±0.76 mm and 2.43±0.54 mm, respectively, and the PPD reduction was 3.29±0.49 mm. There was no significant difference between the two groups.
Changes in the GSH
To evaluate changes in the GSH, 6 groups participated in this evaluation (n=273).
Changes in the GSH according to gingival biotype
Changes in the GSH according to the gingival biotype are displayed in Table 3. In GS-n and GS-k, the GSHs were 0.64±0.42 mm and 0.56±0.37 mm, respectively. In GD-n and GD-k, the GSHs were found to be 0.88±0.45 mm and 0.77±0.45 mm, respectively. No significant differences between the two groups were observed. GN-n and GN-k were additional classifications to compare the amount of GSH at sites with a PPD of less than 3 mm. The GSHs in these groups were 0.43±0.40 mm and 0.23±0.37 mm, respectively. There were significant differences between the two groups (P<0.05).
Changes in the GSH at interdental and middle sites
For more detailed information, all of the sites were classified into interdental sites (n=182) and middle sites (n=88) to evaluate the GSH separately by site (Table 4).
Interdental sites
In GS-n and GS-k, the GSHs were 0.64±0.41 mm and 0.58±0.37 mm, respectively. In GD-n and GD-k, the GSHs were found to be 0.89±0.47 mm and 0.92±0.41 mm, respectively. In GN-n and GN-k, the GSHs were 0.55±0.45 mm and 0.19±0.53 mm, respectively. All of these groups failed to show any significant differences.
Middle sites
In GS-n and GS-k, the GSHs were 0.63±0.48 mm and 0.38±0.35 mm, respectively. In GD-n and GD-k, the GSHs were 0.83±0.37 mm and 0.39±0.31 mm, respectively. In GN-n and GN-k, the GSHs were found to be 0.31±0.27 mm and 0.26±0.28 mm, respectively. All of these groups failed to show any significant differences.
DISCUSSION
The present study aimed to demonstrate whether gingival biotypes can influence the results of SRP, specifically, the PPD and GSH at post-SRP. There were no significant differences between the thin and thick biotypes except the GSH in the GN-n and GN-k groups.
Since gingival biotypes were first advocated in the 1980s as a way of characterizing the gingiva for predicting treatment outcomes and choosing a treatment approach, numerous studies have been conducted on gingival biotypes for various purposes. However, to our knowledge, most of these studies have been limited to establishing the role of gingival biotype in outcomes of surgical periodontal therapy. Therefore, the present study based on the SRP was meaningful because it was focused on predicting the outcomes of nonsurgical therapy.
In the present study, the gingival biotype and PPD change after SRP did not show a relationship. The labial gingiva of the maxillary anterior area showed similar PPD reduction regardless of gingival biotype. In comparing the PPD evaluated separately at the interdental and middle sites after SRP, no significant differences were shown between baseline and 3 months after SRP. This means that other factors may have a greater impact than gingival biotype on the outcomes of SRP. Such factors may include the three-dimensional morphology of the alveolar crest, remained calculus and plaque, and individual healing potential.
These results were similar with those of a previous study that compared PPD reduction after SPR according to GT in a shallow pocket (≤3.5 mm) [15]. In the bleeding and inflammatory group, there were no significant differences of PPD reduction between the thin gingiva (0.4±0.7 mm) and thick gingiva (0.6±0.7 mm) at 3 months after SRP. However, this previous study only analyzed shallow periodontal pockets, while the present study included periodontal pockets of various depths.
It is generally believed that when thin gingiva is violated mechanically, greater shrinkage occurs than when the same is done to thick gingiva. In addition, Fu et al. [13] proposed differences in the tissue reaction with each biotype, such that the thick gingiva is more prone to resulting in a periodontal pocket and the thin gingiva, in GSH after any type of trauma. Pontoriero and Carnevale [4] assessed soft tissue rebound after a CLP according to the gingival biotype. Twelve months after CLP, the amount of soft tissue rebound was significantly more pronounced in the thick biotype both on interproximal and buccal/lingual sites as compared to the thin biotype. Soft tissue around the implant also showed different healing patterns according to the gingival biotype. Cosyn et al. [16] reported more frequent GSH after immediate implant treatment in the thin biotype. Moreover, the thick biotype tended to achieve a pink esthetic score on peri-implant mucosa [17]. In early and conventional implant treatment conducted by Cosyn et al. [18], the thin biotype represented less papilla regeneration. Differences in papilla regeneration according to the gingival biotype after a single implant in the anterior maxilla were investigated by Chou et al. [19]. With a thick biotype, the percentages of interproximal papilla fill after 6 months at the mesial and distal sites were 97%±5% and 94%±8% while the thin gingival biotype showed 53%±9% and 43%±14%, respectively. Considering these results, it is worth noting that thin gingiva is sensitive to any type of surgical periodontal treatment.
However, in the present study, there were no differences in the GSH in groups with a PPD over 3 mm. Only GN-n and GN-k, which represented normal gingival crevices, showed a significant difference, in which the thin gingiva had more GSH than the thick gingiva, and this could be interpreted in relation to the critical probing depth of nonsurgical therapy. In a previous study, Claffey and Shanley [15] noted that thin gingiva and thick gingiva with a PPD of less than 3.5 mm failed to show significant differences on gingival recession with bleeding. In our study, however, thin gingiva and thick gingiva without bleeding also showed no significant differences in GSH.
Various factors, such as bucco-lingual GT, shape of the gingiva, papilla height, and crown form have been used in previous research to distinguish between gingival biotypes [20]. In the present study, only GT measured at 2 mm apical from the gingival margin by CBCT was a reference because the other features mentioned before were found to be less reliable than GT in distinguishing between gingival biotypes.
The thickness threshold most commonly used in other studies to distinguish between thick and thin biotypes is 1.0 mm [21-23]. However, Claffey and Shanley [15] evaluated the effect of GT on periodontal inflammation and set a reference point at a 1.5-mm gingiva thickness. Gingiva with PPD over 3 mm do not tend to maintain a healthy scalloped gingival margin. As we performed experiments on gingiva with a PPD over 3 mm, a GT of 1.5 mm was set as a standard to distinguish between the gingival biotypes in the present study.
Some studies have introduced methods including visual inspection, visualization of a probe through the sulcular margin, direct measurement, and an ultrasonic measurement device [24-29]. CBCT is a reliable method for measuring GT. The CBCT used in the present study was sufficient to distinguish soft tissue in D mode.
In the present study, 3-month re-evaluations were taken to assess GSH and PPD. Lindhe et al. [9] evaluated periodontal parameters at 6 months after SRP with professional tooth cleansing. Stahl et al. [10] reported that 30 days of healing was necessary for complete reconstruction of the periodontal tissue after mucoperiosteal flap surgery. Badersten et al. [12] demonstrated that most GSH took place in the first 2-3 months and remained stable after this period. In the present study, 3 months after SRP, re-evaluation was carried out.
Most of the gingiva in the present study showed gingival swelling caused by supragingival calculus and plaque. To exclude distortion in assessment of PPD and GSH, supragingival scaling was always performed 2 weeks before baseline to eliminate gingival swelling.
By means of assessment of GSH, oral photographs were used at baseline and 3 months after SRP. For additional distortions that were difficult to adjust in the clinic, a computer-aided image program was used to minutely adjust the photographs.
This prospective, controlled study suggested that the roles of gingival biotype in GSH and PPD after SRP were undefined in cases of periodontitis. Gingiva with a PPD over 3 mm failed to show a particular tendency in GSH and PPD by biotype. Only the gingiva with a PPD of less than 3 mm showed more GSH in the thin biotype than the thick biotype. The interdental and middle sites of each group also did not show any particular tendency according to gingival biotype. More studies will be needed to clarify the factors affecting the results of SRP.





 XML Download
XML Download