

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
For many years, dental implants have been widely used to restore missing dentition [1]. The success of the implant is dependent on the nature of osseointegration, the firm bonding between natural bone and the implant [2]. Several studies have established that the surfaces of the implants play an important role in the bone apposition around implants [3-6]. Many studies have concluded that implants with a rough surface showed superior bone formation compared to implants with a smooth surface [7,8]. Various methods for increasing the roughness of the implants' surface have been introduced, including acid etching of the titanium surface, blasting with other solid materials, and coating of biocompatible materials [9]. Calcium phosphate (CaP) is used as a material for modifying the surface in order to improve osseointegration of titanium implants. CaP is known to have characteristics such as enhancing rapid fixation and direct bonding of the implant to bone [10]. However, using coated implants is still controversial because of the coating layer's potential separation from the base material and interference with successful osseointegration by surface degradation. Therefore, various methods for CaP coating have been used, such as plasma spraying, flame spraying, and dip coating [11]. Notably, ion beam assisted deposition (IBAD) has been shown to produce a superior bonding strength between titanium and CaP [12,13]. Primary stability is achieved with initial rigid fixation of implants and is considered essential for a successful treatment outcome. The slightest ability for movement of the implant in the initial stage of healing is regarded to be hazardous. Nevertheless, in some cases within normal surgical protocol, clinicians fail to achieve primary stability due to deficient bone quality or quantity. To overcome this, biocompatible and osteoconductive implants are essential. To evaluate the osteoconductivity of implants with various surface structures, a surgically created circumferential gap defect model has been used [14,15]. Osteoconductivity is evaluated by histologic and histometric analyses of the bone formation around the implants. There are two different processes of bone formation around implant sites, contact osteogenesis and distant osteogenesis. Contact osteogenesis is where new bone forms in direct contact with the implant surface and distance osteogenesis is when new bone forms on the surfaces of the parent bone [16,17]. Both processes participate in closing the defects between the implant and native bone. Specifically for the gap defect model, investigators can discover both processes through histologic observation. In the present study, a histologic and histometric analyses of bone apposition on the surfaces was conducted to evaluate the osseointegration of CaP-coated implants in dogs with or without primary stability.
MATERIALS AND METHODS
Implant surface preparation
Titanium implants (grade IV) were sandblasted using alumina particles and then acid etched by hydrochloric acid. CaP thin film (-500 nm) was deposited on sandblasted, large-grit, acid-etched titanium by an electron-beam deposition system. An electron beam evaporator (Telemark, Battle Ground, WA, USA) at 7.5 kV and 0.13 A, and an end-Hall type ion gun (Commonwealth Scientific, Alexandria, VA, USA) at 90 V and 2.0 A were employed for deposition. Heat treatment after the deposition was conducted at 450℃ in the vacuum of 3 Torr, mmHg. The thickness of the deposited CaP layer was measured by a surface profiler (Model P-10, Tencor, Santa Clara, CA, USA). Evaporants of CaP were prepared by sintering the mixed powder of hydroxyapatite (Alfa Aesar, Johnson Matthey, London, UK) and calcium oxide (Sigma-Aldrich Co., St. Louis, MO, USA) at 1,000℃ for 2 hours.
Animals
Five male mongrel dogs, 18 to 24 months old and weighing about 30 kg, were chosen. All of the animals had intact dentition and healthy periodontium. Animal selection, management, preparation, and surgical procedures followed a protocol approved by the Animal Care and Use Committee, Yonsei University Health System, Seoul, Korea.
Experimental design
The implants were classified into two groups by existence of initial stability: rotational implants (RI) and control (C). Each group was then classified into different healing periods of 4 or 8 weeks. To evaluate the effectiveness of plasma processing, bone-to-implant contact (BIC) and bone density (BD) in histologic samples were measured.
Surgical protocol
All surgical procedures were performed under general anesthesia in a sterile operating room. The animals received an intravenous injection of atropine (0.05 mg/kg; Kwangmyung Pharmaceutical, Seoul, Korea) and an intramuscular injection of xylazine (2 mg/kg; Rompun, Bayer Korea, Seoul, Korea) and ketamine hydrochloride (10 mg/kg; Ketalar, Yuhan, Seoul, Korea). Local infiltration anesthesia was also performed using 2% lidocaine hydrochloride (Lidocaine, Kwangmyung Pharmaceutical) followed by inhalation anesthesia using 2% enflurane (Gerolan, Choongwae Pharmaceutical, Seoul, Korea). All mandibular premolars and the first molar were extracted and allowed to heal for 8 weeks. The implants were then placed under the same edentulous conditions as extraction of teeth. A midcrestal incision was performed to make a mucoperiosteal flap on the left side of the mandible. The implant site was prepared using surgical drills in both groups (RI, C). We used the same CaP-coated implants in all of the groups, but the method for preparing the site differed in each group. The final drill used in the RI group was 3.4 mm in diameter, the same as that of the implant, which allows for relatively free movement of implants in surgical sites after surgery. On the other hand, in the C group, we gave rigid fixation of implants using smaller final drills with diameters of 2.85 mm. All mucoperiosteal flaps were sutured with glyconate monofilament (Monosyn 4.0, B.Braun, Tuttlingen, Germany), and the implants were maintained in a submerged state for the whole healing period. To generate a different healing time, the same procedures were performed on the right side of the mandible 4 weeks later. All of the animals were sacrificed with an anesthesia drug overdose 8 weeks after the first surgery. The specimens acquired were fixed in 10% neutral buffered formalin for 10 days.
Specimen preparation
Specimens were dehydrated in ethanol, then embedded in methacrylate, and sectioned in the buccolingual plane using a diamond saw (Exakt, Apparatebau, Norderstedt, Germany). From all of the block sections, the central section was reduced to a final thickness of about 20 µm and processed by hematoxylin-eosin staining. Histometric analysis using a stereomicroscope (MZFLIII, Leica, Wetzlar, Germany) and microscope (DM-LB, Leica) was done followed by general histologic observation. An automated image-analysis system (Image-Pro Plus, Media Cybernetics, Silver Spring, MD, USA) was used for histometric analysis.
RESULTS
Clinical findings
During the experimental period, all of the implants were well-maintained and healing was uneventful. There were no active signs of inflammation or complications including wound dehiscence, swelling, or bleeding in the mucosa adjacent to the implants.
Histologic findings
Four-week group
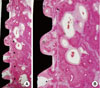
Newly formed bone was observed along the threads of the implants. In the RI group, reversal lines indicating implant ostectomy were observed away from the threads (Fig. 1). Most of the gap areas between the threads were filled with new bone. There was no specific histologic difference between the two groups (Figs. 1 and 2).
Eight-week group
In the 8-week group, woven bone along the threads of the implants was replaced by mature lamellar bone and well-organized osteons were observed. Many primary and secondary osteons were seen within the thread area when compared with the 4-week group. The bone marrow contained adipocytes, vessels, collagen fibers, and some mononuclear leukocytes. A thin rim of newly formed bone apparently covered most of the rough surface in the bone marrow compartment (Figs. 3 and 4).
Histometric analysis
The histometric analysis results of all 20 implants are presented in Figs. 5 and 6. The mean BIC and BD showed a slight increase in the RI group, and a tendency toward a decrease in the control group over time. However, there were no statistically significant differences in BIC and BD between the two groups.
DISCUSSION
A dental implant is an optimal treatment option for various clinical conditions. Following an extraction of a tooth, the alveolar bone undergoes complicated stages of healing [18]. This creates a challenging situation for clinicians to obtain primary stability of the implant. Several options have been utilized to address this issue, including alveolar ridge splitting, modifying the drilling method, and use of wide implants. As osteoconductivity of the implants is essential for the success of these procedures, a variety of surface modifications to the implant have been developed and adjusted. In a systematic review of newly developed and marketed oral implants, Junker et al. [7] reported that modifying the procedures for deposition on the surface of the implants can affect the chemical composition of oral implants. They concluded that sufficient proof of a safe and predictable implant-to-bone response is related to surface roughness. A review of experimental surface alterations revealed that CaP-coated implants can improve osseointegration compared to non-coated titanium implants. Despite promising clinical results, a relatively long treatment time frame is required for dental implants when compared to conventional dental prostheses including fixed crowns and removable dentures. To shorten the time spent restoring missing dentition, the concept of an immediate implant was introduced [19], but the primary stability in the immediate implant is much harder to achieve because of discrepancies arising between the dimensions of the natural teeth and implants. To solve this clinical problem, several studies have suggested methods that evaluate the degree of osseointegration using different methods of analysis. Stadlinger et al. [20] reported that majority of in vivo studies used histological and histomorphometric methods although the location of the implant and animals used differed among the studies. Results of the histometric analysis tend to increase with time while results of the radiographic assessment decreased. In the present study, an oversized-drilled model was used to evaluate the osteoconductivity of implants coated with CaP using IBAD. Despite the different healing periods and different methods of implant site preparation, all implants were successfully osseointegrated. The results of this study are in agreement with a study performed by Chae et al.[21]. They obtained a rapid formation of new bone that was in contact with the implant by coating the implants with nano-sized CaP. Previous studies have revealed that implants installed without mobility exhibited a higher BIC value in the early healing phase, and maintained it. On the other hand, the mean BIC value in the rotationally mobile implants increased gradually according to time [22]. Song et al. [23] compared two different modified surfaces of implants using gap defect models and Um et al. [24] compared different postcoating heat treatment methods [24]. CaP layers coated using the IBAD technique provided high bond strength between implants and natural teeth. In addition, cell adhesion to the implant surface improved in a histologic observation [23]. A postcoating heat treatment can also affect the cell attachment to implant surfaces by increasing the crystallinity of the coated surface [24]. These advantageous characteristics lead to firm and direct bonding of the implants to the bone. This might play an important role in achieving consistency of osseointegration. Further clinical studies in humans evaluating osseointegration with a standardized protocol could provide a theoretical background that could be applied to clinical practice.
In conclusion, within the limitation of this study, successful osseointegration of CaP-coated implants could be achieved under unfavorable conditions without primary stability. CaP coating using IBAD could be an effective method for the surface treatment of dental implants.





 XML Download
XML Download