

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The term "endo-perio" lesion has been proposed to describe the destructive lesions resulting from inflammatory products found in varying degrees in both the periodontium and the pulpal tissues [1]. Endo-perio combined lesions include pulpal disease with secondary periodontal involvement (primary pulpal lesion), periodontal disease with secondary endodontic involvement (primary periodontal lesion), and true combined lesions [2]. As teeth with primary pulpal disease with secondary periodontal involvement and true combined lesions have already lost their vitality, endodontic treatment would be the best treatment option [3]. In the case of periodontal disease with secondary endodontic involvement, some teeth demonstrate necrotic pulp whereas others still retain their vitality [2].
Deep periodontal intraosseous lesions with secondary endodontic involvement usually occur when the downward progression of a periodontal pocket reaches the periapical tissues [4]. Primary periodontal lesions with secondary endodontic involvement generally end up with a resultant pulpal necrosis as they progress apically, yet the pulp often remains vital [2]. The reason is that even when pathologic changes occur in the pulp tissue influenced by destructive periodontal disease, the pulp usually does not undergo the degenerative process as long as the main canal is not affected [5]. Furthermore, although the pulp may demonstrate histologic evidence of inflammation, the potential for maintaining pulpal vitality remains if the main blood supply is not compromised [6]. Therefore, the treatment modality of primary periodontal lesions with secondary involvement of an endodontic lesion has been controversial.
In 1980, Casullo [7] classified combined endo-perio lesions into five categories and proposed that periodontal treatment alone be applied to periodontal disease with secondary endodontic involvement based on its periodontal origin. Gold and Moskow [6] have observed that an alternative treatment using both surgery and antibiotics without any concomitant endodontic therapy resulted in successful outcomes. Extensive damage to the periapical tissues may be treated without devitalizing a tooth if the lesion is of periodontal origin and properly diagnosed [5]. There is consensus among these studies that primary periodontal lesions should be managed only with periodontal therapy and, because of its origin, endodontic therapy would be unnecessary.
However, Bender and Seltzer [8] found that, among a group consisting of 57 teeth with periodontal disease but without caries or fillings, 79% of teeth showed pathological changes within the pulp. Such an untreated endodontic infection may influence the outcome of periodontal wound healing, leading to a higher risk of attachment loss [9]. As a result, pulpal conditions can influence marginal healing and repair as long as the affected dentinal tubules remain patent [10]. Without initial endodontic treatment, the exposure of dentinal tubules by the removal of cementum by rigorous scaling and root planning during the course of periodontal treatment will allow bacterial invasion of the tubules. This would increase the likelihood of cumulative damage to the pulp. Therefore, nontoxic intracanal therapeutic medicaments may be necessary to eliminate the bacteria and to help encourage tissue repair [1]. In summary, initial proper endodontic management can prevent pulpal infection and facilitate regenerative potential.
In the present study, patients who exhibited radiolucency extending to the periapical region, abnormal electric pulp testing values, and deep probing depth derived from primary periodontal disease with secondary endodontic involvement were included. We propose endodontic treatment prior to periodontal regenerative treatment for those teeth with secondary endodontic involvement in which communication with an apical lesion is present although the teeth remain vital.
CASE DESCRIPTION
This study protocol was approved by the Pusan National University Dental Hospital Institutional Review Board (#PNUDH-2013-012).
Case 1
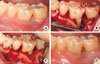
A 57-year-old male who had a chief complaint of dull pain in the upper right first premolar visited the Department of Periodontology, Pusan National University Dental Hospital. There was no remarkable systemic disease. A wide radiolucent lesion on the upper right first premolar was evident with a probing depth of 9 mm only in the palatal surface. The electric pulp testing result demonstrated a positive value (+8). The tooth was diagnosed as a primary periodontal lesion with secondary endodontic involvement based on the positive electric testing value with a wide periapical radiolucent lesion and deep probing depth. Accordingly, an intentional endodontic treatment plan was proposed, followed by regenerative periodontal treatment. At 3 months following the commencement of the intentional endodontic treatment, the palatal probing depth remained deep and a wide radiolucent lesion was still evident due to the untreated primary periodontal lesion. Regenerative periodontal treatment was scheduled to address the intraosseous defect without concern as to whether pulpal infection by periodontal treatment would occur. Upon flap reflection, an anorganic bovine bone (BBP, Oscotec Inc., Seoul, Korea) graft was placed into the lesion following palatal root debridement. Follow-up was performed every 3 months for 1 year. A radiographic image taken 1 year postoperatively showed a significant decrease in radiolucency suggestive of remarkable enhancement of the bone density around the affected region (Figs. 1 and 2).
Case 2
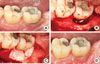
A 55-year-old female presented with swelling and pus discharge on the labial aspect of the lower left first molar. The tooth had degree 1 mobility and was modestly positive (+7) according to the electric pulp test. The probing pocket depth was 10 mm at the distal sites. Radiographic images showed a wide and deep radiolucent lesion around the distal root. The diagnostic impression was a primary periodontal lesion with secondary endodontic involvement judged by the positive electric testing value with the wide periapical radiolucent lesion and deep probing depth. The treatment plan consisted of initial endodontic treatment followed by regenerative periodontal treatment. The swelling and pus discharge subsided after the endodontic treatment and root planing; however, the deep pockets on the distal root area remained given that the primary periodontal disease had not yet been fully managed. Regenerative periodontal therapy was scheduled to fill in the remaining defects following the endodontic treatment. Open flap debridement with an anorganic bovine bone (BBP) graft was performed and the intraosseous lesion healed uneventfully. Nine months following the surgical intervention, the radiographic images showed significant bone filling around the distal aspect of the distal root. The optimal level of occlusal function was restored and the patient was satisfied with the final outcomes (Figs. 3 and 4).
Case 3
A 33-year-old male visited our periodontal clinic with a chief complaint of persistent dull pain on the lower left second molar on chewing and biting. The clinical condition was characterized by deep pocket depths ranging from 9 to 12 mm on the midbuccal and distal area, without a noticeable mobility or suppuration upon gentle probing. The result of the electric pulp tests indicated that the second molar was vital (+7), and the radiographic image revealed a circumferential radiolucency surrounding the distal root apex. The diagnostic impression was a primary periodontal lesion with secondary endodontic involvement based on a positive electric testing value with a wide periapical radiolucent lesion and deep probing depth. Intentional endodontic treatment followed by regenerative periodontal treatment was planned. Three months after the endodontic treatment, the guided tissue regeneration was performed for the resolution of the primary periodontal intraosseous lesion. The guided tissue regeneration consisted of the placement of a nonresorbable (expanded polytetrafluoroethylene) barrier membrane (Goretex, W.L. Gore and Associates, Newark, DE, USA) with anorganic bovine bone (BBP) graft. The membrane was removed at 6 weeks postoperatively. The lesion healed uneventfully and a radiograph taken at more than 6 months following the regenerative surgery demonstrated remarkable osseous repair and an enhanced radiopacity (Figs. 5 and 6).
DISCUSSION
Pulpal and periodontal tissues communicate with each other via various pathways such as the vascular system, apical foramen, and lateral canals. These patent foramina and canals can be potential communication routes of endodontic-periodontal inflammation [11]. The similarity in the composition of cellular infiltrates also implies the connection between the pulp and periodontal tissues. Taken together, these findings can support the notion of cross-contamination between the pulp and the periodontal tissues [12].
Periodontal inflammation may initially elicit degenerative change in the pulp. However, partial necrosis of the pulp may render a positive pulp testing value despite the existence of a combined lesion, especially in a multirooted tooth [13]. This is because the pulp usually does not undergo degenerative changes unless the main canal is involved, even when pathologic changes occur in the pulp derived from periodontal inflammation [5].
Some authors have warned that untreated endodontic infection can influence periodontal healing, with a higher risk of attachment loss [9]. The success rate of the endo-perio combined lesion without a concomitant regenerative procedure has been reported to range from 27% to 37% [14]. This result demonstrates the notably low success rate and explains why regenerative periodontal surgery should be performed following endodontic treatment in combined endo-perio lesions.
Proper diagnosis and adoption of the bone graft technique or the guided tissue regeneration technique combined with osseous grafting followed by the removal of etiological factors will only ensure complete restoration of the health and function to a tooth with severe attachment loss resulting from a combined endo-perio lesion [15,16]. Britain et al. [17] showed that management of induced endo-perio lesions by bioabsorbable collagen membranes alone or in combination with anorganic bovine bone matrix resulted in enhanced amounts of bone and periodontal ligament and significant increases in the amount of new cementum when compared to open flap debridement alone.
Many authors have claimed autogenous bone grafting to be the graft of choice for regenerative procedures [18]. However, a significant amount of bone regeneration is achievable with a xenograft and it removes the limitations of harvesting a sufficient amount of autogenous bone.
In the present case report, intentional endodontic treatment was performed prior to regenerative periodontal treatment in teeth with a positive electric pulp testing value that seemed abnormally high. We concluded that degenerative and necrotic changes of the pulp that had progressed due to long-standing periodontal inflammation despite the positive pulp testing value may suggest that the pulp was not totally necrotic. Regenerative periodontal treatment was scheduled to address the remaining intraosseous defect only after osseous healing was induced sufficiently by initial endodontic treatment. Although the target teeth in the present case report were diagnosed as having primary periodontal lesions with secondary endodontic involvement, intentionally scheduling an initial endodontic treatment could help reduce pain and prevent undesirable secondary pulpal infection during regenerative periodontal surgery. Following an intentional endodontic intervention, anorganic bovine bone grafts or guided tissue regeneration with a nonresorbable barrier membrane could successfully resolve an extensive intraosseous defect extending to the periapical region. Within the limitations of the present observations, an intentional endodontic intervention is proposed as a potential approach for the sophisticated management of teeth suffering from serious attachment loss and alveolar bone destruction with concomitant secondary endodontic involvement.




 XML Download
XML Download