

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Over the past few decades, dental implants have become one of the most effective treatments following tooth loss. However, there has been controversy about marginal bone loss around dental implants since screw-type implants were first introduced in 1971-specifically, whether the bone loss is caused by pathologic change or a normal biologic response.
Peri-implant diseases were recently classified into two groups at the 6th European Workshop on Periodontology in 2008: peri-implant mucositis and peri-implantitis [1]. Both types of peri-implant diseases were confirmed as infections [1-3] associated with the development of biofilm [4,5]. A recent study found that 28% of subjects with dental implants had progressive bone loss [6]. Treatments proposed for the management of peri-implant diseases have been largely based on the data available about the treatment of periodontitis [7]. The rationale is to keep the bacterial load below the individual's threshold for disease. To achieve this goal, mechanical debridement using hand or ultrasonic devices, adjunctive use of chemical agents, and laser application have been used for nonsurgical treatment of peri-implant mucositis and periimplantitis [8]. However, although peri-implant mucositis was found to be reversible by nonsurgical therapy [9], periimplantitis remained problematic [1]. A previous study evaluating the effects of combined surgical and antimicrobial interventions on peri-implantitis found that 7 out of 26 implants were lost despite repeated treatment [10].
Developments in surface modifications have allowed for enhanced osseointegration of implants, but they might also enhance biofilm formation [7], so the exposed and contaminated rough surface of these implants could not be restored completely by conventional treatments. For these reasons, the prevention of peri-implant disease (including periodontitis) is more important than the treatment of disease progress. The principal objective of preventive therapy for periodontal/peri-implant diseases is suppressing bacterial colonization via mechanical plaque control, and ultrasonic devices have commonly been used in clinical applications for periodontal preventive treatment due to their effectiveness. However, while conventional mechanical instruments can plane a diseased irregular root surface, they also roughen the surface of a titanium implant surface [11,12]. In order to overcome some of these limitations, non-metallic devices or other alternative methods have been developed for the maintenance treatment of dental implants, including [13-17] plastic curettes, air-powder abrasion, and a specially-designed ultrasonic system (Vector, DÜRR DENTAL AG, Bietigheim-Bissingen, Germany). However, several recent studies have revealed their weaknesses, including inadequate effects or toxicity of their remnants [18-20].
Therefore, the present study used a newly developed metal ultrasonic scaler that is softer than titanium so as to avoid damaging the implant surface. The objectives of this study were to 1) determine the effects of the various ultrasonic scaling systems with different degrees of hardness on changes to the titanium surface, and 2) estimate the changes to titanium surfaces according to the angle at which the instruments are applied.
MATERIALS AND METHODS
Materials and study design
Thirty-seven pure titanium disks 5 mm in diameter (Dentium, Seoul, Korea) were used in this study. They were divided into the following 5 groups according to the different instruments used (Table 1, Fig. 1):
Groups 1, 2, and 3 were further subdivided into two groups in which two tip angles (15 and 45 degrees) were applied. This produced, a total of eight groups (including the control group), each of which included five disks.
Experimental procedure
Two small lines were scribed as orientation marks onto each surface: the lines were approximately 2 mm long and separated by 2 mm (Fig. 2). The titanium surfaces were treated and then examined in this area. The titanium surfaces were cleaned with a solvent wash of acetone for 1 minute before and after each hygiene treatment, and then air-dried and wrapped in 2×2 gauze. The specimens were oriented horizontally on a table, and the piezoelectric conventional scalers were used at moderate finger pressure for 30 seconds at 15 and 45 degrees, 25 kHz, and at their highest power. The piezoelectric root planer was applied at 27 to 32 kHz at its highest power (Fig. 3). The plastic hand curette was used at finger pressure for 30 strokes at 45 degrees. Untreated titanium surfaces served as controls. All experimental procedures were performed by the same investigator.
Scanning electron microscopy
Titanium specimens were examined by scanning electron microscopy (SEM; S-300OH, Hitachi, Tokyo, Japan) operating at 10 kV and photographed at a magnification of ×200. Before examination, the specimens were coated with an electroconductive layer of gold, which was evaporated by an ion sputter coater (E 101, Hitachi).
Profilometer
After scaling, the surface roughness of the specimens was assessed with a profilometer (CS 3100, Mitutoyo, Tokyo, Japan). This instrument measures high-frequency surface irregularities and not widely-spaced irregularities caused by waviness or curvature.
The average surface roughness (Ra) and the mean roughness profile depth (Rz) were measured. In each case, the measurement was performed with a 0.25 mm cutoff and over an assessment length of 1.25 mm. Each specimen was measured three times at 0.5 mm intervals lengthwise and widthwise, from which the average for each specimen was calculated.
Statistical analysis
Individual mean values were calculated. A one-way analysis of variance was used to evaluate the differences between the titanium surfaces, and the post-hoc Scheffe's test was used to evaluate differences between groups. A P-value of <0.05 was considered significant. SPSS ver. 12.0.0 (SPSS Inc., Chicago, IL, USA) was used for all of the statistical analysis.
RESULTS
SEM observations
The characteristics of the titanium surfaces in the obtained SEM images varied with the applied treatment. It was evident that the untreated disks did not have smooth surfaces with circumferential milling marks being evident (Fig. 4A).
The use of the plastic hand curette (PH group) (Fig. 4B) and the newly developed metallic scaler tip (NS group) (Fig. 4C and D) did not appear to markedly affect the titanium surfaces, although some smoothening occurred. The surface roughness did not differ among the NS, control, and PH groups.
The use of the piezoelectric conventional scaler (CS group) (Fig. 4G and H) and piezoelectric root planer (PR group) (Fig. 4E and F) clearly resulted in scraping of the titanium surfaces and loss of their original texture, leading to increased surface roughness.
In addition, the SEM images demonstrated that the changes in the surface texture were less extensive when the procedure was performed at 45 degrees than at 15 degrees. However, there were no statistically significant differences between these two experimental groups.
Profilometer analysis
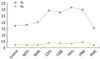
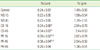
The roughness parameters in the experimental and control surfaces (mean values of Ra and Rz) are reported in Fig. 5 and Table 2.
All of the procedures increased the roughness parameters, except for treatment with the plastic hand curette (PH group: 0.20±0.04 µm, mean±standard deviation) and the newly developed metallic scaler tip (NS group: 0.22±0.05 µm for the 15 degree group and 0.23±0.06 µm for the 45 degree group), which showed a lower Ra value than the control one (0.24±0.07 µm). The Ra values for the titanium surfaces increased following treatments with the piezoelectric conventional scaler tip (CS group) and root planer (PR group) at 15 and 45 degrees (0.34±0.06 µm or 0.34±0.03 µm and 0.39±0.02 µm or 0.36±0.04 µm). There were statistically significant differences between the NS and PR groups (P<0.05) (Table 2).
Most of the procedures increased Rz (1.59±0.54 µm, 2.54±0.79 µm, 2.82±0.78 µm in the NS, CS, and PR group): the exception was treatment with the plastic hand curette (PH group: 1.38±0.51 µm). Rz was lower in the PH group than in the control group (1.49±0.50 µm) (Fig. 5, Table 2). There were no statistically significant differences.
DISCUSSION
Compromised oral hygiene resulting in plaque accumulation is a major risk factor that can contribute to the failure of dental implants, and hence good oral hygiene is one of the prerequisites for the long-term success of implants [21,22]. The principal objective of treatment of peri-implantitis is complete removal of all calcified and bacterial deposits from implant surfaces in order to stop disease progression. Many studies have investigated the effects of using different hygiene instruments on dental implant surfaces [12,13,23-26]. Routine prophylactic procedures might cause damage to implant surfaces over time and lead to changes in the surface topography that can increase the potential for plaque accumulation.
Quirynen et al. [27] reported that any metal-to-metal contact might lead to a damaged implant surface during professional cleaning [28]. This has led to many instruments being developed that aim at less damage to the titanium surface: these incorporate Teflon-coated, plastic, or other types of nonmetallic tips [26,29,30]. However, the application of nonmetallic instruments has been reported to be inadequate for eliminating bacteria from roughened implant surfaces [11,24]. Air-powder abrasive systems have also been introduced for cleaning contaminated implant surfaces [11,31], but their applications are limited by being associated with an increased risk of emphysema [32]. Schwarz et al. [18] also reported that a nonmetallic carbon fiber tip (Vector ultrasonic scaler) was not suitable for decontaminating titanium surfaces. Titanium surfaces treated with the Vector system showed conspicuous surface damage and deposits of the used carbon fibers, with a reduction in the cell density on all implant surfaces.
The present study used an ultrasonic scaler with a newly developed metallic scaler tip composed of copper alloy and plated with 99.99% silver. Because the newly developed scaler tip (89HV) was softer than the titanium fixture (200 to 280HV) and conventional scaler tip (610HV), its use would reduce or even avoid damage to the implant surface during treatment of peri-implantitis [33]. Therefore, the present study compared the effects on titanium surfaces of the newly developed scaler tip with those of a plastic hand curette and piezoelectric ultrasonic scalers.
In a result of this study, the effects on the titanium surface were minor in the PS and NS groups but significant in the CS and PR groups (Fig. 4). The SEM analysis revealed that the plastic hand curette (PS group) and the newly developed metallic scaler tip (NS group) produced no changes to the titanium surface topography (Fig. 4B-D). SEM showed that the plastic hand curette (PH group) produced similar results to those of previous studies that have employed plastic scalers [24-26]. Severe surface changes were observed following treatment by the conventional scaler tip (CS group) and piezoelectric root planer (PR group) (Fig. 4E-H), which is in accordance with the result of studies by Cross-Poline et al. [14] and Hallmon et al. [15]. Samples in the PR group, in which a root planer with a conventional scaler tip was used, showed deep surface abrasions on the titanium surfaces in SEM analysis (Fig. 4E and F).
A profilometer is a direct-reading instrument for measuring the average roughness height down to the micron levels. Two basic amplitude parameters were used in this study to characterize the implant surface roughness: Ra and Rz. Ra is universally recognized and the mostly commonly used parameter of roughness: it corresponds to the arithmetic mean of the absolute deviation of the roughness profile from the mean line determined by fitting a least square line of nominal form through the primary profile. Rz corresponds to the maximum peak-to-valley height of the profile over the assessment length.
In this study, the roughness increased in the CS and PR experimental groups compared with the control group, while there was a small reduction in the Rz value when using a plastic curette or the newly developed metallic scaler tip (Fig. 5). These results are in accordance with previous studies finding that the Ra and Rz values after using nonmetallic scaler tips were similar to or lower than those in the control groups, whereas the use of the metallic scaler tip increased both Ra and Rz [16,28,29].
Another objective of the present study was to identify an appropriate application method of a scaling system for treating peri-implantitis, which was achieved by measuring changes in the titanium surface according to the angles between the scaler tip and the surface. There were no significant differences between the results of SEM and profilometer analyses. The changes in or damage to titanium surfaces might be affected more by the hardness of the scaler tip than by the application method.





 XML Download
XML Download