

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dental implants have been successfully used for replacing missing teeth with reported success rates of more than 90% [1,2]. Improvements in the surface and design of dental implants have contributed to this remarkable success rates. Recent advances in the radiographic techniques used in implant dentistry have increased the accuracy of presurgical planning [3,4]. However, there exist the risks of nerve injury and maxillary sinus perforation originated from inappropriate presurgical planning due to innate discrepancy between radiographic measurements and real dimensions. Precise radiographic assessment of available alveolar bone and identification of characteristic bone morphology are indispensible for dental implant placement. When posterior maxillary and mandibular sites are considered, the location of important anatomic structures such as the mandibular canal and maxillary sinus should be identified carefully for proper implant site selection and length selection.
Pain or paresthesia caused by inferior alveolar nerve injury is one of major complications. Another major complication is maxillary sinus inferior wall perforation which is known to be correlated with the incidence of infection followed by failure of a dental implant [5,6]. Therefore, special care should be taken not to invade important anatomic structures during surgery when presurgical planning is made based on radiographs. More precise radiographic techniques and corresponding proper computer programs to guide precise surgery would reduce the complication rate [4]. Presurgical planning is mostly made with radiographs such as panoramic, lateral cephalometric, and periapical radiographs, and computed tomography (CT) [7,8]. However, none of these types of radiography represents a perfect modality [9,10]. More accurate radiographic technique is required, especially for presurgical planning in areas where important anatomic structures are located. Finding an appropriate location and measuring the available bone based on panoramic radiograph is one of the most frequently used modalities for presurgical planning. A panoramic radiograph displays the body of the mandible and maxilla, mandibular canal, and maxillary sinus on a single image. The length and mesiodistal angulation of an implant are usually determined in the panoramic radiograph. However, in the anterior area where more distortion exists than posterior area, the reliability of panoramic radiographs for presurgical planning of an implant is questionable [11-13].
The necessity of cross-sectional imaging for a dental implant has been emphasized [14,15]. According to the recommendation from American Academy of Oral and Maxillofacial radiology in 2000, cross-sectional images including conventional spiral tomography, linear tomography, or CT should be used for presurgical planning [16]. These cross-sectional imaging techniques exhibit various accuracies. Linear tomography is reported to be significantly less accurate than spiral tomography in detecting mandibular canal [17]. However, it was reported that measuring available bone volume only using spiral tomography may lead to a dangerous situation because the available vertical bone height is exaggerated in spiral tomography relative to panoramic radiography [12]. CT provides less magnification than the other types of cross-sectional tomography. The magnification in CT corresponds to 0 to 4% [18]. CT can offer direct volumetric reconstruction. Faster and easier data transformation into three-dimensional analysis is possible. In addition, convenient interpretation is also possible without overlapping of images [17]. However, one major disadvantage of CT is a high radiation dose [19], and therefore cone-beam CT (CBCT) was developed to overcome this limitation [20,21]. CBCT images are known to have higher quality than CT images with 1/400 radiation dose of conventional CT [19,20].
Each type of radiograph has its own advantages and disadvantages. Therefore, the radiation dose, magnification rate, and specific indications need to be considered when selecting the type of radiographic images to use in presurgical planning. The purpose of this study was to determine the reliability of presurgical planning based on the use of two types of radiographic image (digital panoramic radiography [DPR] and CBCT) by beginner dentists to place implants.
MATERIALS AND METHODS
Study design
Ten fresh cadavers without posterior tooth were used to examine the accuracy of CBCT and DPR measurements. These cadavers were from persons who donated their bodies for research or teaching purposes. The posterior teeth were extracted when there is not any missing posterior tooth. Twelve dentists who never had any experience of implant surgery were participated in implant surgery after 10 hours of basic instruction not including hands-on training. Thereafter, each participant performed implant surgery using a conventional surgical guide based on CBCT or DPR on their own. The sites for implant surgery were randomly assigned for the two investigated presurgical planning methods: 31 implants were placed with the surgical guide based on DPR and the corresponding computer program (Starpacs, Infinitt Co., Seoul, Korea), while 32 implants were placed with the surgical guide based on CBCT and the corresponding computer program (Ondemend 3D, Cybermed Inc., Seoul, Korea).
Two types of measurement error were evaluated in this study: 1) The presurgical measurement error: difference between the presurgical and postsurgical measurements in radiographs. 2) The measurement error: difference of measured distances between postsurgical radiographs and the cadaver specimens.
Measurement errors for CBCT
Virtual planning to determine the appropriate length of the implant was first performed using CBCT and the corresponding program. D1 was the difference between the distance from the implant platform to the anatomic structure (e.g., inferior wall of the maxillary sinus or superior border of the mandibular canal) and the distance from the implant platform to the implant apex. D2 was the distance from the implant apex to the anatomic structure in postsurgical CBCT. D3 was the distance from the implant apex to the anatomic structure in the real specimen. The presurgical and postsurgical measurement errors for CBCT were calculated by subtracting D2 from D1 and subtracting D3 from D2, respectively. These measurements are illustrated Figs. 1-3.
Measurement errors for DPR
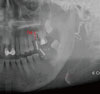
Virtual planning to determine the appropriate length of the implant was performed using DPR and the corresponding program. A presurgical panoramic radiograph was obtained to measure the distance from the implant apex to the anatomic structure (D4), which was the difference between the distance from the alveolar ridge to the anatomic structure and the planned implant length. D5 was the distance from the implant apex to the anatomic structure in postsurgical DPR. D6 was the distance from the implant apex to the anatomic structure in a real cross-sectioned specimen. The presurgical and postsurgical measurement errors for DPR were calculated by subtracting D5 from D4 and subtracting D6 from D5, respectively. These measurements are illustrated Figs. 4 and 5.
RESULTS
Presurgical measurement errors
The mean presurgical measurement error was significantly smaller for CBCT than for DPR (P≤0.05) (Table 1). The presurgical measurement error was significantly smaller for CBCT (1.26±1.23 mm) than for DPR (3.32±2.34 mm, P=0.008) in the maxillary region, whereas it did not differ significantly between the two imaging modalities in the mandibular region (1.58±1.25 mm vs. 2.32±1.81 mm, respectively, P=0.164) (Table 2).
Measurement errors between postsurgical radiography and real specimens
The measurement error between postsurgical radiography and cadaver specimens was significantly smaller for CBCT than for DPR (P≤0.05) (Table 3). This difference was statistically significant in the maxillary region (P≤0.05) but not in the mandibular region (1.65±1.24 mm vs. 1.06 ± 0.55 mm, P=0.098) (Table 4).
Critical errors
Some specimens experienced critical errors such as maxillary-sinus invasion, mandibular-canal invasion, and lingual-plate perforation (Fig. 6). The error rate in the implant surgery was higher in DPR than in CBCT.
DISCUSSION
Statistically significant differences in measurement errors were found between the two radiographic techniques in the present study. This result is consistent with that of previous studies [22,23]. The errors were greater for DPR than CBCT because presurgical plans are made on a two-dimensional plane for DPR. CBCT should be used for presurgical planning and postoperative evaluation, especially when dentists with limited experiences place implants, considering the reduced errors in three-dimensional presurgical planning.
The measurement errors in the maxilla were significantly lower for CBCT than DPR. It can be attributed to the difficulty of identifying the exact location of the inferior wall of the maxillary sinus in presurgical planning when using DPR. Various levels of the inferior border of the maxillary sinus are overlapped in DPR. To the contrary, the exact levels of the inferior border of the maxillary sinus can be identified using CBCT because the view in the specific plane where the implant will be placed is used for presurgical planning. These data suggest that presurgical planning using DPR for implant placement on the maxillary premolar or molar area is not sufficiently reliable. Even though limitation of DPR can be compensated by abundant clinical experiences, more accurate and precise methods are recommended for preventing unexpected complications.
In mandible, the measurement error in CBCT didn't show any statistically significant difference from that in DPR. This result is in accordance with that of one previous study [11]. This shows that there will be fewer errors when presurgical plans are made using DPR in mandible than maxilla. Identifying the superior border of the mandibular canal is easier than the inferior border of the maxillary sinus because the mandibular canal is easy to identify in most cases, except those with thick cortical bone or a high proportion of trabecular bone. This convenient detection of the mandibular canal can allow dentists to place implants in the posterior mandibular area without any critical complications as long as the buccolingual width is measured carefully. Direct measurement using calipers is recommended intraorally or extraorally in a study cast. In summary, presurgical planning in the mandible can be performed safely using DPR by dentists with sufficient experience and skill, whereas presurgical planning using CBCT is strongly recommended when a buccolingual location of the mandibular canal needs to be evaluated.
Radiographic images do not always display anatomic structures accurately. In maxilla, it was revealed that less measurement errors between postsurgical radiographic images and real specimens were found in CBCT than DPR. More accurate detection of the inferior wall of the maxillary sinus was possible using CBCT.
Both positive and negative presurgical measurement errors were obtained, whereas only positive measurement errors were obtained between postsurgical radiographs and real specimens. It appears that the distance from the implant apex to anatomic structures was always greater in a postsurgical radiograph than in the corresponding real specimen.
This study has revealed the best radiographic methods to use in order to reduce errors by beginner dentists during dental implantation. Future studies should evaluate the validity of computer-assisted implant surgery with a surgical guide fabricated based on CBCT. In addition, it is necessary to evaluate the measurement errors when experienced dentists are placing implants.








 XML Download
XML Download