

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
During the past two decades, interest has been growing in scientific circles in establishing a relationship between periodontal diseases and pregnancy problems [1]. Several studies have shown a relationship between periodontal diseases and premature birth and infant low birth weight (LBW). For example, an animal study has shown that periodontal disease results in LBW [2]. In addition, animal studies have shown the mechanism of LBW due to periodontal diseases. Collins et al. [3] showed that animals with periodontal disease have high blood levels of chemical mediators that lead to uterine contractions, dilatation of the uterine cervix, labor pains, and finally abortion. Human studies, too, have compared LBW and immature newborns between healthy mothers and mothers suffering from periodontal diseases. Some of these studies have shown such a relationship. Offenbacher et al. [4] reported a seven-fold higher risk of premature delivery and LBW in mothers with periodontal disease than in healthy mothers. However, some other studies have not shown such a relationship. Davenport et al. [5] did not report a higher risk of LBW in mothers with periodontal disease. Some other human studies have evaluated pregnant women and have compared the outcomes of pregnancies in mothers with and without periodontal diseases. The preliminary results of these studies showed that mothers with periodontal disease have a higher risk for premature deliveries [6,7]. Offenbacher et al. [7] reported a relationship between the severity of periodontal disease and LBW and premature birth. However, some other studies have not shown a relationship between the severity of periodontal disease and LBW and immature newborns [8,9]. Some other interventional studies have shown that the risk of LBW and immature newborns decreases with the treatment of periodontal diseases [10,11].
According to the definition of the World Health Organization an immature newborn is a newborn delivered before a gestational age of 37 weeks with a birth weight of less than 2,500 g [12]. On the other hand, immature birth is multifactorial and factors of both the mother and the newborn might contribute to it [11,13]. Based on the definition above, prematurity cannot always be associated with severe somatic problems in the newborn and a more accurate index is required to determine the complications of preterm delivery in the newborn. However, several studies have shown that LBW and immaturity of the newborn might result in enamel hypoplasia in the deciduous and permanent dentitions [14].
Despite the wide range of studies aimed at determining the relationship between the periodontal disease of the mother and preterm birth and LBW, and regardless of the success or failure of showing such a relationship, no studies have so far evaluated the effect of the mother's periodontal disease at the time of delivery on the vital indexes of the newborn.
An Apgar score is a rapid test that is carried out at 1- and 5-minute intervals after delivery. Designed in 1952 in Colombia by Dr. Virginia Apgar, the test comprises evaluating the newborn's heart rate, respiration, muscular tonicity, excitability reflexes, and skin color, and each item receives a score of zero, 1, or 2 based on the situation observed. At 1-minute intervals the Apgar score evaluates the tolerance to the delivery process and at 5-minute intervals it evaluates the adaptation of the newborn to the environment [15].
The aim of the present study was to evaluate the relationship between the periodontal diseases of mothers and the condition of their newborns by using the Apgar score in an attempt to determine whether the mother's periodontal disease can have an effect on the infant or not.
MATERIALS AND METHODS
In the present descriptive case-control study, the subjects were selected from the pregnant women referred to the Gynecology and Obstetrics Center of Tabriz University of Medical Sciences. All of the subjects were in their third trimester of pregnancy. A total of 100 pregnant women with periodontal disease and 100 pregnant women without periodontal disease, who were matched in relation to age and socioeconomic status, were selected.
The inclusion criteria
The exclusion criteria
A total of 100 pregnant women with periodontal disease were assigned to the test group. The same number of pregnant women who were matched in relation to age, socioeconomic status, and gestational age with the subjects in the case group but did not have periodontal disease were assigned to the control group. None of the subjects had a history of systemic conditions. Based on the Third National Health and Nutrition Examination Survey (NHANES III) index [16], periodontal disease consists of one or several periodontal areas with attachment loss of >3 mm and pocket depth of >4 mm. In the NHANES III periodontal examination, half of the patient's teeth are examined. One quadrant from the maxilla and one quadrant from the mandible are randomly selected. The distance from the gingival margin to the floor of the sulcus (probing depth [PD]) and the distance from the gingival margin to the cemento-enamel junction (CEJ) are determined for each tooth at the mid-facial and mesio-facial aspects. Attachment loss is determined by measuring the distance from the CEJ to the floor of the sulcus, which is measured with the use of a Williams probe and a dental mirror. The periodontal parameters were recorded in special forms, and after the baby was born, the baby's Apgar score was added to the forms for statistical analysis. Periodontal parameters of clinical attachment loss (CAL), PD, and bleeding on probing (BOP) in mothers with and without periodontal disease were evaluated and recorded. An unpaired Student's t-test was used to analyze differences in means between the case and control groups using SPSS ver. 13 (SPSS Inc., Chicago, IL, USA).
The medical files of the newborn babies were used to record their weight, age in weeks, gender, and Apgar score.
An odds ratio (OR) was used to determine the relationship between the infants with Apgar levels of <7 and periodontal disease. In addition, Pearson's correlation coefficient was used to evaluate the correlation between the infant's Apgar values and the periodontal parameters in the mothers with and without periodontal diseases.
RESULTS
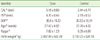
Table 1 presents the means of age, periodontal PDs, attachment loss, the areas with BOP, Apgar scores in the first 5 minutes, and birth weights in the case and control groups. As the table shows, all of the variables exhibited statistically significant differences between the case and control groups except for age.
The risk OR of an Apgar score of <7 with a mother with periodontal disease was calculated to be (OR, 3.14; 95%; P=0.24) at a confidence interval (CI) of 1.08 to 9.11.
On the other hand, the risk of LBW in patients with periodontal disease was calculated by comparison of the risk of LBW in mothers without periodontal disease (OR, 2.74; 95% CI, 1.18 to 6.35; P=0.013).
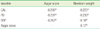
In addition, Pearson's correlation coefficient between the weight of the newborn baby and mother's BOP, CAL, and PD and the correlation coefficient between the Apgar score and mother's BOP, CAL, and PD and also the correlation coefficient between the Apgar score and newborn's birth weight were calculated (Table 2).
DISCUSSION
The results of the present study showed infant birth weight means of 2,962.02±502.89 and 3,193.22±528.18 g in the case and control groups, respectively; the means of Apgar scores were 7.82±1.23 and 8.35±0.88 in the case and control groups, respectively. Statistical analysis showed significant differences between the case and control groups in relation to birth variables.
Although no studies have been reported to date on the correlation between the Apgar score and periodontal diseases and it has been shown that the Apgar score itself has a high level of positive correlation with infant birth weight [17], it might be possible to correlate the results of infant weight to the results of Apgar scores.
The results of the present study in relation to infant birth weight are consistent with those of other studies in this regard [6,10,11]. On the other hand, some other studies have rejected such a correlation [5,8,9]. Michalowicz et al. [18] carried out an interventional study in 2006 and reported that periodontal treatment has no effect on infant birth weight or an increase in Apgar value [18].
The results of the present study showed that mothers with periodontal diseases, compared to mothers without periodontal diseases, gave birth to infants with lower birth weights, with statistically significant differences between the two groups (P=0.002). In addition, the risk of birth weight of <2,500 g in mothers with periodontal disease was (OR=2.74; 95%; P=0.013) with a CI of 1.18 to 6.35. The results of the present study were consistent with the results of a study by Offenbacher et al. [19]. They reported the risk of birth weight of <2,500 g in mothers with periodontal disease to be (OR, 2.4; 95%; P=0.01) with a CI of 1.1 to 5.2.
In contrast, Offenbacher et al. [7] reported in 2001 that the risk of LBW in African-American women was 7.9. One year later, Davenport et al. [5] reported that African-Americans are potentially at risk of bearing infants with LBW. The differences in the risks reported in the present study and those reported by Offenbacher et al. [7] in 2001 might be attributed to the fact that their study included only African-American mothers with periodontal diseases, resulting in an increase in the odds of babies born with LBW. However, the results of a study by Jeffcoat et al. [20] are almost consistent with those of the present study (3.5; 95% CI, 11.7 to 7.3) and slight differences might be attributed to the number of subjects, disease severity, or racial differences [20]. However, some studies have rejected any relationship between periodontal disease and LBW [21]. In contrast, some interventional studies have shown this relationship, indicating that treatment of periodontal disease can decrease the risk [11].
Shirmohammadi et al. [22] showed that a decrease in the newborn's body size was observed as the mother's periodontal disease severity increased. Birth weight, height, and head and chest circumferences of babies born to mothers with established periodontal disease were significantly lower than those who were born to mothers with healthy periodontium, gingivitis, and initial periodontal disease (P=0.006, P=0.016, P<0.001, and P<0.001, respectively).
In the present study the correlation coefficient between LBW and Apgar value on one hand and periodontal parameters of BOP, CAL, and PD are presented in Table 2, all of which indicate a strong correlation. Offenbacher et al. [7] reported this correlation to be (r=0.49; P<0.01); however, Meurman et al. [23] reported it to be much higher (r=0.59; P<0.01). In the present study, the correlation coefficient between birth weight and CAL was (r=0.22; P<0.01). Therefore, the differences in the correlation coefficients reported in several studies, including the present study, might be attributed to the conditional correlation between oral health parameters and the different outcomes of pregnancy in different populations.
Although the results of the present study and other similar studies or interventional studies indicate the relationship between periodontal diseases and a decrease in Apgar score and immature births, and some interventional studies have shown that periodontal treatment in pregnant women is without any risks and improves the mother's periodontal status, some other studies have indicated that periodontal treatment of the mother has negative effects on the fetus. Goepfert et al. [24] detected the mother's periodontal pathogens in 2 cases out of 44 cases in the placenta and 3 of the mothers they evaluated had premature births. The results of that study reflect the theory that periodontal pathogens, especially Porphyromonas gingivalis and Campylobacter rectus, reach the placenta through the bloodstream, the membranes, and the amniotic fluid, leading to premature birth and LBW infants [1]. Therefore, the important question of "whether rendering phase I treatment during pregnancy can give rise to bacteremia and subsequent infiltration of periodontal pathogens into the placenta or not" should be answered because some studies have shown an improvement in the birth weight and an increase in Apgar value and some others have not shown any such evidence. Considering the results of the present study and other studies in this respect, it is suggested that during prenatal health programs, it should be emphasized that before deciding to have babies, mothers should receive dental treatments, including periodontal treatment.
 XML Download
XML Download