

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Apical shift of gingival marginal tissues beyond the cemento-enamel junction (CEJ) is known as gingival recession and is a common disease [1]. It is one of the major esthetic and functional concerns cited in the literature [2,3]. Due to the consequences of gingival recession, such as tooth hypersensitivity [4], caries, compromised esthetics, and reduction of the attached gingiva [5], periodontists are searching for a new method to overcome this problem. Different surgical techniques have been assessed such as the laterally positioned flap [6], coronally positioned flap (CPF) [7], free gingival graft [8,9], and subepithelial connective tissue graft (SCTG) with a CPF [10]. The connective tissue graft with a CPF is considered to be the gold standard for root coverage (RC) due to its high predictability [11-13]. Recently, there has been an increasing interest in the potential applications of growth factors for enhancing wound healing through naturally occurring biological pathways. Logically, it seems plausible to utilize plasma rich in growth factors (PRGFs) as a natural growth factor composite to enhance the healing properties of various human wounds. Studies in wound healing have shown that platelets that are involved in clot formation after surgery release some growth factors that play a role in cell proliferation and differentiation; therefore, they contribute a major role in tissue healing and formation [14]. Platelets have an intrinsic supply of vascular endothelial growth factor (VEGF), which may be released when the platelets are stimulated or aggregated by collagen. It has been demonstrated that transforming growth factor (TGF)-β2 and TGF-β1 trigger rapid maturation of collagen in the early wound healing process. Platelet-derived growth factors (PDGFs) increase the population of wound healing cells and recruits other angiogenic growth factors to the wound site [15]. A new technique for preparing the platelet concentrate is the PRGF system. The advantages of this system over platelet rich plasma (PRP) is the fact that PRGF is less time consuming, does not require bovine thromboplastin for activation, requires less venous blood, the product is devoid of white blood cells and inflammatory interleukins, and centrifugation may be performed in only one step [16].
PRGF is a mixture of PDGF, TGF-β, and VEGF. These chemical mediators play a significant role in the wound repair process [16,17]. PRP was first introduced into dentistry through maxillofacial surgery. However, the use of PRP has been suggested for periodontal regenerative procedures. Most of the previous studies have focused on the effects of growth factors on bone healing [18-21], but limited evidence exists on their effects on soft tissue healing [1,22]. Due to the advantages of PRGF over PRR, as mentioned in our previous study [23], we evaluated the clinical efficiency of PRGF when applied as an adjunct to coronally advanced flap (CAF) and found that PRGF enhanced the outcomes of CAF especially throughout the first month postoperatively. The aim of the present study was to determine whether the application of the PRGF to the SCTG enhances RC significantly.
MATERIALS AND METHODS
This study was designed as a randomized, blind, split-mouth trial. It was conducted between August 1, 2007 and June 10, 2009 in the Department of Periodontics of the Tabriz Dental Faculty. Ten patients with twenty sites of bilateral Miller's class I or class II were selected [24]. The inclusion criteria included a minimum 3 mm of vertical gingival recession depth (RD) on the incisors, canines, or premolars located in the contralateral quadrants of the same jaw in the maxilla or mandible. An adequate vestibular depth was a prerequisite for accomplishing the CPF [25].
The exclusion criteria were history of any systemic diseases that could influence the periodontium or grafting prognosis, bleeding on probing in the surgical area, restoration on the test or control teeth, plaque index (PI) greater than or equal to 20%, pregnancy, taking drugs that are known to interfere with wound healing such as corticosteroids or anticancer agents, history of RC in the test or control teeth, indications for antibiotic prophylaxis, patients who did not sign the informed consent, smoking, deep frenal attachment, history of coagulant disorders, or taking drugs that are known to interfere with platelet activity such as non-steroidal anti-inflammatory drugs (NSAIDs).
The study design was approved by the Ethics Committee and was supported by the Research Deputy of Tabriz University of Medical Sciences. The nature of this investigation was explained in detail to the patients, and the patients signed an informed consent form.
The test group received SCTG plus PRGF, and the control group received SCTG without PRGF. The sites were randomly selected by flipping a coin for the control or test group immediately before surgery. A flowchart of the study participants is presented in Fig. 1.
Preoperative stage
All the subjects received oral hygiene instructions and supragingival scaling prior to the study. In a blind manner, one calibrated examiner made pre- and postmeasurements. The primary efficacy parameters for the study were RD, the distance between the CEJ to the free gingival margin at 3 months. The secondary efficacy parameters included the width of keratinized tissue (WKT), which was measured as the distance from the mucogingival junction (MGJ) to the free gingival margin, the clinical attachment level (CAL), which was assessed as the distance from the CEJ to the apical end of the gingival sulcus in the midpalatal region, and the clinical pocket depth (PD), which was measured as the distance from the CEJ to the apical end of the gingival sulcus midbuccal point of the purposed teeth. Moreover, the position of the MGJ was measured as the distance from the CEJ to the MGJ in the midfacial region of the purposed teeth, the gingival index (GI) was recorded as suggested by Loe [26], and and the PI was recorded according to the Silness and Loe PI system [27]. All of the clinical parameters were measured using a Williams periodontal probe (Hu-Friedy, Chicago, IL, USA). The RC percentage was calculated using the following formula:
([Preoperative RD - Postoperative RD]/Preoperative RD) ×100.
The final parameters were taken at 1 and 3 months postoperatively by the same examiner who was still blind to the method of the study.
PRGF preparation
The preparation of PRGF was performed immediately before surgery as described by Anitua and Andia [28]. Prior to the surgery, 10 mL of venous blood was collected from the subjects. The blood was kept in 5 mL tubes with 3.8% trisodium citrate as an anticoagulant (Fig. 2). The tubes were centrifuged at 1,800 rpm for 8 minutes at room temperature (PRGF System II, BTI, Vitoria-Gasteiz, Spain). As a result of centrifugation, the blood was compartmentalized into the following four components (Fig. 3):
Plasma poor in growth factors (PPGFs) in the upper portion of the tube and corresponding to a volume of 0.5 mL.
Plasma with growth factors (PGFs) comprising approximately 0.5 mL of the total volume.
PRGF (0.5 mL) located immediately above the red blood cell fraction in the tube.
Red blood cell concentrate.
The PPGF located in the upper part of the plasma in the tube was eliminated with 500 µL pipettes. PPGF has the lowest quantity of platelets in the plasma. The functional fraction is usually 0.5 mL of PRGF located immediately above the red blood cell fraction. The PRGF was separated with 500 µL pipettes and transported to an independent tube. Next, the PRGF was activated using 50 µL of 10% calcium chloride. The mixture of PRGF and calcium chloride was left at room temperature for 10 min, until a consistent and easy to handle gelatinous layer had formed (Fig. 2).
Surgical procedure
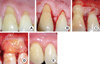
All of the patients were treated by the same surgeon. The exposed root surfaces were scaled and planed with hand and ultrasonic instruments. After local anesthesia with lidocaine 2%+epinephrine 1:80,000, two horizontal incisions were made 2 mm below the papillae on both sides of the affected tooth, and then two vertical incisions were made extending beyond the MGJ. Mesiodistally, the flap should be at least half a tooth wider than the lesion width. A partial thickness flap was then reflected. A SCTG was obtained from the palate using a horizontal incision 5 to 6 mm from the gingival margin of the molars and premolars. The connective tissue was then trimmed of the adipose and glandular tissue [10]. A PRGF gel was placed over the root surface, and the SCTG was placed over the gel and immobilized using resorbable sling sutures (Fig. 4). The recipient flap was then sutured over that with silk sutures. The area was covered with a surgical pack (Coe-Pak, GC America Inc., Alsip, IL, USA). Intermittent ice pack application was used immediately after surgery and for the first 24 hours at the control and test sites for 20 minutes per hour. All of the subjects were advised to discontinue any mechanical oral hygiene measures for 4 weeks and to avoid any trauma to the surgical sites. The patients were instructed to rinse twice daily for 4 weeks with a 0.2% solution of chlorhexidine gluconate (Shahr Darou Laboratories, Tehran, Iran). Ibuprofen (400 mg three times a day; Hakim Pharmaceutical Co., Tehran, Iran) was prescribed for postoperative pain, and amoxicillin (500 mg three times a day) was administered for 10 days. The sutures were removed 10 to 14 days after surgery. The patients were followed weekly during the first month, and then monthly thereafter until the end of the study. Follow-up sessions included removal of supragingival plaque and reinstruction on oral hygiene. All of the parameters were measured after 1 and 3 months.
RESULTS
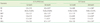
All of the 20 patients, aged 40 to 50 years, finished the study. During the evaluation period no side effects were reported, except transient edema immediately after surgery. During the 3 months after treatment, all the patients maintained excellent levels of oral hygiene, and the plaque and GI did not demonstrate any significant differences compared to the baseline values (P>0.05). The baseline, first month, and third month evaluation data are presented in Table 1. The comparison of baseline parameters did not show any significant difference between the test and control groups (P>0.05).
Intra-group comparisons (Table 1)
The RD for the test group (SCTG+PRGF ) was an average of 2.7 mm (77%) and 2.6 mm (74%) lower than the baseline values in the first and third month evaluations after surgery, respectively (P=0.004). For the control group (SCTG), the RD reduced to about 2.4 mm (70%) at 1 month and 2.2 mm (64%) at 3 months, which were significantly lower than the baseline values (P=0.004). Between the first and third month, the RD increased 0.1 mm (2%) in both groups.
The WKT revealed a 1.1 mm (22%) and 0.8 mm (16%) increase in the test group, in the 1st and 3rd month evaluations, respectively. This change was statistically significant compared to the baseline values (P=0.01). There was a 0.3 mm decrease in WKT between the first and third months in the test group. In the control group, the WKT revealed a 1 mm (21%) and 0.8 mm (17%) increase in the 1st and 3rd month evaluations, which were significantly higher than the initial measurements (P=0.03). However, a 0.2 mm (4%) reduction occurred between the 1st and 3rd month values.
The CAL also showed significant changes in both the test and control groups. A 2.8 mm (59%) attachment gain at 1 month and a 2.7 mm (57%) attachment gain within 3 months occurred in the test group, which were significant changes compared to the baseline values (P=0.004). In the control group, a 2.6 mm (54%) attachment gain occurred at 1 month , and it remained unchanged up to the third month. This change was significant compared to the initial measurements (P=0.004). There was no mean gain of attachment in the control group between the first and third month; on the other hand, a 0.1 mm (2%) attachment loss was observed in the test group during this period.
The PD was relatively stable regardless of the treatment. The PD did not show any significant change compared to the baseline values (P>0.05) in both the 1st and 3rd month measurements.
In the test group, the MGJ increased about 1 mm (16%) between the baseline and first month (P<0.05), and it increased 0.7 mm (11%) between the baseline and third month (P<0.05). In the control group, the MGJ increased 0.8 mm (13%) between the baseline and first month (P<0.05), and it increased 0.5 mm (8%) between the baseline and third month. A 0.3 mm (5%) reduction was observed between the first and third month.
Inter-group comparisons (Table 2)
The test group showed a greater decrease, an average of 0.2 mm (5%), in RD than the control group in both the first and third month evaluations. However, this finding was not statistically significant.
The amount of RC in the test group averaged 78.33% after 1 month and 75.83% after 3 months. In the control group, these values were 74.18% and 70.85%, respectively. However, the differences in both the first and third month values between the two groups did not reach statistical significance.
The mean increase of WKT in the test group was 0.2 mm (4%) greater than in the control group. Likewise, in the third month, the test group reached a WKT of 0.1 mm (2%) more than the control group, but these inter-group differences were not statistically significant.
Similarly, the CAL in the test group gained 0.3 mm (6%) more attachment than the control group in the first month, and the test group also gained 0.2 mm (4%) more attachment than the control group in the third month. These values did not reveal any statistically significant differences between the two groups.
As mentioned previously, the PD was not affected by the treatment options.
The mean increase of the MGJ in the test group was 0.1 mm (1%) greater than in the control group in the first and third month evaluations, but this difference was not statistically significant.
DISCUSSION
Many researchers have attempted to improve the existing RC techniques. One possible way to improve the clinical results of this treatment is to use growth factors. Most of the studies in this field, have investigated the effects of PRP on RC procedures [1,22]. PRGF is the end product of a new system for obtaining platelet growth factors, and PRGF has unique advantages such as reduced preparation time (15 to 20 min is required for PRGF preparation compared to a minimum of 30 minutes for PRP preparation) and needing less venous blood volume (at least 5 mL) compared to PRP (50 to 500 mL). Furthermore, plasma separation in PRP preparation requires two high-speed centrifugation steps (5,600 rpm and 2,400 rpm) compared to a single low-speed centrifugation step (1,800 rpm) in the PRGF technique. Centrifugation at a high-speed in two stages activates a number of platelets, but in the PRGF technique, the platelets are 100% inactive. PRGF preparation does not require bovine thromboplastin for activation. This fact might be an advantage because it has been shown that the application of thrombin stimulates the production of anti-thrombin antibodies, resulting in controversy in its utilization [16].
The predictability of RC is a main consideration in selecting the treatment method for gingival recession. This study evaluated the efficiency of SCTG with and without PRGF in treatment of Miller's class I and II gingival recession defects. The results of the two techniques were encouraging. In our study, the two techniques improved all of the parameters except for PD. Although the amount of improvement in SCTG+PRGF was slightly better than SCTG only, this difference was not statistically significant, which is in agreement with some previous studies [1,22,29]. The postoperative measurements were performed 1 and 3 months after treatment. Although the important changes observed in the first month were generally preserved up to the third month, a tendency to relapse to the presurgical measurements was seen. This may be due to the control of the etiologic and patient factors such as soft tissue contraction and early false positive postoperative results caused by postoperative inflammation and edema [30].
In the present study, the mean reduction of the RD was 2.6 mm (74%) and 2.3 mm (64%) in the SCTG+PRGF and SCTG groups, respectively. Huang et al. [22] examined the efficiency of PRP plus CAF in the treatment of Miller's class I gingival recession. They found that the RD was reduced to 2.4 mm in CAF and 2.3 mm in CPF+PRP. The initial mean of their study was 2.9 mm and 2.8 mm, respectively. Despite the higher amount of RD and the inclusion of Miller's class II defects in our study, we obtained similar or even slightly better RD corrections. This might have been due to the use of SCTG, the shorter follow-up intervals, and the higher baseline mean of KWT in the present study. Pini Prato et al. [31] suggested that increased flap tension results in diminished RC. In the present study, the baseline mean of WKT was 4.8 mm in the SCTG+PRGF group and 4.7 mm in the SCTG group, which actually reflected our inclusion criteria. In the study by Huang et al. [22], WKT was 2.7 mm; therefore, the tension on the flaps we performed seems to have been less than in the previously mentioned study. Again, in the Huang et al. [22] study the inter-group difference was not statistically significant, just as in our study.
We achieved a mean RC of 75% and 70% in the SCTG+PRGF and SCTG groups, respectively. The inter-group difference was not significant. These findings are similar to some previous studies [1,29]. Huang et al. [22] reported a mean RC of 83.5% in the CPF+PRP group, which was greater than what we achieved in our study. The higher RC might have been due to a more favorable and predictable RC of the Miller's class I defects compared to the class II defects.
Several studies have demonstrated successful results of CTG in the treatment of buccal gingival recessions [12,29,32]. Slight differences between the results might have been due to the different case selections, biomaterials used, and follow-up duration.
WKT is a critical factor for maintenance of gingival health. In the present study, a significant increase in WKT was observed in the SCTG+PRGF and SCTG groups. The WKT increase of 1.2 mm was found in the two groups after 3 months. Similar findings have been reported in studies that incorporated CTG [22,32-34]. On the other hand, Jankovic et al. [29] reported that CTG+PRP is advantageous over CTG for increasing the WKT. The growth factors from PRP may have a positive effect on the proliferation of gingival and periodontal fibroblasts. It should be kept in mind that CPF, on its own, has a positive effect on the WKT because of the biological activity of granulation tissue derived from periodontal ligaments [35,36].
A recent systematic review investigated the effects of autogenous platelet concentrates on the clinical outcomes of surgical treatment for periodontal diseases and found no added adjunctive role for the platelet concentrate for treating gingival recessions [37]. PRGF also did not seem to have any effect on the RC parameters of the group treated with CAFs without SCTG [23]. The clinical attachment gain in the SCTG+PRGF and SCTG groups were 3.3 mm and 2.6 mm, respectively, which were similar to previous study results [1,29]. Although some studies have reported significantly higher readings [38], they were probably due to the use of collagen membranes with the purpose of guided tissue regeneration.
In our study a 0.1 mm and 0.2 mm recession occurred in the SCTG+PRGF and SCTG groups, respectively. This change was not significant, namely the PD remained constant throughout the study. This finding is in agreement with most of the studies [1], but not all of them [38]. The diversity of the PD readings can be explained in two ways. First, it could be due to the different techniques used in the studies. Second, the initial amount of PD is different among the studies, and this makes outcome comparisons impossible. All of this aside, we used a certain technique described by Anitua and Andia [28] to prepare the PRGF, which is advantageous over other techniques because it includes only one-step centrifuge instead of two-step centrifuge and does not need bovine thrombin; moreover, less blood volume is needed [16].
Additional research with more cases and longer follow-up periods combined with histological studies is suggested for evaluating the effects of PRGF on the healing process and the persistence of the results, is recommended.
In conclusion, the present study suggests that the treatment of gingival recession with SCTG+PRGF or SCTG only results in clinically favorable outcomes. However, there was no significant additional effect of PRGF. The disadvantages of PRGF application include complexity in preparation and handling of PRGF during surgery, increased surgical time, and patient discomfort.




 XML Download
XML Download