

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In 1981 Albrektsson et al. [1] emphasized the bio-compatibility, morphology, surface treatment, condition of recipient site, surgical technique, and control of loading condition as key factors of successful osseointegration in dental implants. They also reported other factors needed for successful implant therapy such as patient selection, experience of the surgeon, initial stability of the implant, placement timing, esthetics, and responsiveness to the grafting material [2-5]. Clinically, obtaining sufficient initial stability is crucial. This depends on the bone density of the surgical site, the surgical method, and the microscopic surface characteristics and macroscopic morphology of the implants [6].
Among various factors in predicting the success of implant therapy, factors determined by the patient are the volume and density of available bone [7,8]. The atrophy of available bone after extraction limits the length and diameter of the implant. Initial stability is weakened by decreased bone density, which in turn affects implant success. Many previous studies have shown that placement of short implants due to severe bone loss at the implant site resulted in an increased failure rate. Bone density is usually decreased after tooth loss and this also has an effect on implant success [9-12].
Assuming an acceptable level of surgeon's experience and patient's bone quality, reliable implants will result in a more predictable outcome. Therefore, the success rate of implants in the implant system is considered a measure of reliability. Since Schnitman and Shulman [13] proposed success criteria for implants, several criteria have been proposed [14,15], and the report by Albrektsson et al. [16] is most widely used.
However, recent studies have been conducted on implants with immediate placement or early-loading protocols. It is difficult to compare the two types of studies in analyzing their survival or success rates. Carr et al. [17] reviewed 674 1-stage implants with a 78-month follow-up period. In this retrospective study, the implant survival rate was determined by means of Kaplan-Meier survival estimates. No failures were noted 13 months after placement. Penarrocha et al. [18] reported a 1-year survival rate for a single implant with early loading within 6-8 weeks after placement. Buser's survival criteria [15] and the Kaplan-Meier survival estimates were used to compare these results with the survival rates of other implants with early loading. Many studies have considered 1 year after implant placement to be a critical point because the Kaplan-Meier survival curve almost reaches a plateau 1 year after the implant placement. Performance of bone augmentation did not affect the implant success rate or the amount of marginal bone loss [19-21].
Until recently, various implant systems have been introduced to increase the success rate and research on implant design and surface treatment has been actively performed [22,23]. Many studies have revealed that the success rate is higher in rough-surfaced implants by various surface treatments than in smooth-surfaced implants by machining [24,25]. Regarding the morphology of the implants, the initial stability was enhanced by self-tapping implants and the success rate was also increased [26,27].
The Astra Tech implants reviewed in this study have a microthreaded conical neck and TiO blast surface (Fig. 1) [28]. Microthreads on the fixture top prevent concentration of the stress around the alveolar ridge crest and decrease marginal bone loss [29]. The fixture and abutment are strongly connected at an 11.5 degree angle by the conical seal design. The conical design seals off the connection and decreases micro-movement and micro-leakage [30,31]. In 1998 Norton documented a statistically significant decrease in the bone loss around Astra Tech implants after 4 years of radiographic assessment. Palmer et al. [32] found an average 0.39 mm bone loss in a 5-year prospective study in 2000. Shin et al. [33] documented a smaller degree of bone loss in implants with microthreading regardless of bone quality in a 1-year prospective comparative study in 2003. A statistically significant difference was found, especially in the maxilla.
The aim of this study was to analyze the short-term predictability and reliability of Astra Tech implants according to the demographical distribution of patients and condition of implant sites and location of implants.
MATERIALS AND METHODS
Subjects and materials
Among patients treated with Astra Tech implants in the Department of Periodontology at the Dental Hospital of Yonsei University of College of Dentisry and K Dental Clinic from May 2004 to March 2009, 195 implants in 98 patients which had been restored more than 6 months earlier were reviewed in this study (Table 1).
The intraoral locations of the Astra Tech implants are as shown in Table 2.
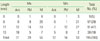
The diameters of Astra Tech implants were 3.5 mm, 4.0 mm, 4.5 mm, and 5.0 mm. The lengths of the implants varied widely, and ranged from 8 mm to 13 mm (Tables 3 and 4).
This study was approved by the Institutional Review Board of Dental Hospital of Yonsei University of College of Dentistry (IRB number 2-2011-0014).
Methods
The following data were reviewed from patient charts: 1) patient type and implant location, 2) bone status at the implant site, 3) diameter and length of the placed implants, 4) presence or absence of bone augmentation and types of the augmentation. The implant success rate was then examined in light of these variables.
Before implant placement, every patient went through oral and radiographic examinations. A medical history was also taken and smoking habits were reviewed. Implants were not placed in patients with an absolute contraindication that could not be controlled. In those patients, the edentulous areas were given an alternative treatment. Patients were also interviewed about the cause and timing of the extraction to determine the types of tooth loss by age and sex.
The bone status at the implant site was documented according to Lekholm and Zarb's classification [11]. Bone quality and bone quantity was evaluated during surgery. The diameter and length of the implants placed were reviewed from the patient charts.
Using the patient charts, the surgical procedures (1-stage or 2-stage implant placement procedure), additional bone augmentation procedures, and graft materials (such as bone or artificial membrane) were reviewed. The time until completion of prosthodontic treatment after implant installation was also investigated. In addition, the follow-up data (including patient interviews and oral and radiographic examinations) older than 6 months after prosthodontic treatment were evaluated.
Assessment method
The survival criteria were based on those proposed by Buser et al. in 1997 and by Cochran et al. in 2002. The criteria includes: 1) the absence of clinical mobility of the implants, 2) the absence of subjective sensitivity or pain, 3) the absence of peri-implantitis, and 4) the absence of persistent radiolucency around the implants.
RESULTS
One hundred and ninety-five implants were evaluated in this study. Regarding implant length, 11 mm was the most common (47%). With respect to the diameter of implants, 4 mm occupied the largest portion (35%), followed by 5.0 mm (30%), 3.5 mm (25%), and 4.5 mm (10%). This is because implant diameter is restricted by the bucco-lingual width of the available bone and the relationship with adjacent teeth [9,34].
Fifty-five implants (28%) were applied using a 1-stage implant placement procedure, and the other 140 implants (72%) using a 2-stage procedure. Also, for 74 implants in surgical sites with poor bone quality or quantity an additional bone augmentation procedure, such as sinus augmentation or the guided bone regeneration procedure, was used. Prosthodontic treatment was completed by 2 to 20 months after implant installation with a mean of 5.9 months.
Survival rate according to implant location
Most implants were placed in the molar area, especially the 1st molar area of the maxilla, and there was no difference in the survival rate according to the implant location (Table 5).
Survival rate according to bone quality
Most implants were placed in D2 and D3 bone types, and there was no difference in survival rate according to bone quality (Table 6).
Survival rate according to bone quantity
Most implants were placed in areas of B and C bone quantity, and there was no difference in survival rate according to bone quantity (Table 7).
Survival rate according to the presence or absence of bone augmentation procedure
An autogenous bone graft, allograft, or alloplast with artificial membrane were used for placement of 74 implants. Maxillary sinus elevation procedures were performed for the placement of 33 implants in the maxillary posterior region. Nevertheless, there was no difference in the survival rate (Table 8).
DISCUSSION
Since the introduction of the concept of osseointegration by Branemark in the early 1960s, implant therapy has been a commonplace for replacing edentulous areas in daily practice. Up to now, implants with various shapes, designs, and surface treatments have been introduced. In the Department of Periodontolgy at the Dental Hospital of Yonsei University of College of Dentisry, 4,500 implants were placed for approximately 10 years from 1992 to 2002, and based on these patient records, basic assessments have been undertaken regarding patient type and distribution of implant location [35]. Among various implant systems, the microthreaded and conical seal design of the Astra Tech implant has shown lower marginal bone loss around implants, as well as less microleakage and micromovement [28-33,36], thus increasing the long term success rate.
In this study, 195 Astra Tech implants were placed in 98 patients in the Department of Periodontolgy at the Dental Hospital of Yonsei University of College of Dentisry and in K Dental Clinic. Based on these data, the short-term survival rate of Astra Tech implants was evaluated by considering bone quality, bone quantity, and bone augmentation procedures.
In 1985, Brånemark et al. [8] classified the bone status around the implant surgery area. This has been used by many clinicians to predict treatment outcomes. In this study, the bone quality and bone quantity were separately evaluated. With respect to bone quality, the predominant bone type was D3 in the maxilla and D2 in the mandible. With regard to bone quantity, type B and C occupied most cases (96%) of the maxilla and type B was predominant in the mandible (73%). We often encounter situations where the bone quantity is deficient in an edentulous area. To place implants with sufficient length and diameter in these areas, a bone graft with autogenous bone or alloplastic material with or without a membrane are required. Additional procedures are also necessary, especially in the maxilla, such as in maxillary sinus elevation. Currently, the development of these procedures has contributed to a high success rate of implants, and implants can be placed in more challenging cases [37].
In 1997, Kemppainen et al. [38] reported that the short-term survival rate of Astra Tech implants is 97.8%, and in 2004, Norton [39] reported that it is 96.4%. In this study, the short-term survival rate was 100% regardless of bone quality, bone quantity, or use of bone augmentation procedures. These high short-term survival rates are due to the distinctive fixture design of the Astra Tech implant, which results in excellent initial bone responses. Therefore, the use of an Astra Tech implant can result in predictably good treatment results even if the bone quality is poor and bone augmentation is necessary because of poor bone quantity.
The patient type, distribution of implant locations, and survival rate of Astra Tech implants were investigated in this study and following was concluded:
The short-term survival rate of Astra Tech implants was 100%.
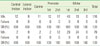
Bone quality was in the decreasing order of D3 (55%) >D2 (28%) >D4 (16%) >D1 (0%) for the maxilla and D2 (77%) >D3 (18%) >D4 (4%) >D1 (1%) for the mandible with a 100% survival rate.
Bone quantity was in the decreasing order of Type B (51%) >C (49%) >D (3%) >A (1%) for the maxilla and Type B (73%) >C (18%) >D (5%) >A (4%) for the mandible with a 100% survival rate.
Bone augmentation was carried out in 38% of implants placed, with 100% survival rate.
Considering the consistent outcomes mentioned above, Astra Tech implants can be reliably used in daily practice. If additional bone augmentation procedures are performed to improve the bone quality and quantity in areas where the bone condition is not optimal, acceptable treatment results can be expected.







 XML Download
XML Download