

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pathologic tooth migration (PTM) is tooth displacement resulting from the imbalance of tooth retention forces [1]. A variety of factors are regarded to be related to PTM, and the incidence is reported to be up to 50% of periodontitis patients [2,3]. The factors are, specifically, destruction of periodontium, inflammation in periodontal tissue, eruption force, oral habit, pressure in soft tissue, and occlusal force. Destruction of periodontium is one of the major causes of PTM, and it is known to make the incidence of PTM 3 to 8 times higher according to the amount of bone loss [2]. Inflammation in periodontal tissue increase hydrodynamic and hydrostatic forces around relevant vessels and tissues, possibly resulting in tooth displacement [4]. Eruption force may be a contributing factor, since extrusion is a common clinical feature of PTM [3]. Various occlusal factors are also related to PTM, as are oral habits such as lip and tongue habits, fingernail biting, thumb sucking, pipe smoking, and bruxism, and pressure from soft tissues like the tongue, cheek, and lips.
Treatment options for PTM are to remove causes and allow for natural healing, to provide limited additional orthodontic treatment after extraction of migrated teeth, and to generally straighten teeth [3]. Clear aligner, which is used for additional or limited orthodontic treatment of PTM, was introduced as a gingival stimulating appliance in 1926 [5], and Kesling [6] reported it to be used for tooth movement. Clear aligner is effective since it intermittently generates 3-dimensional orthodontic force. The protocol starts with applying a 0.5 mm-thick aligner for the first week. The thickness is then increased to 0.75 mm for the next 2 weeks. This procedure relieves patients' pain and decreases undesirable effects on the neighboring teeth with gradual teeth movement of 1 mm at each stage [7]. However, due to its elasticity and deformation, the appliance has to be remade every three weeks. Clear aligner might be indicated for a small amount (≤4 mm) of teeth movement, for instance, space closure, extrusion and intrusion, arch expansion and contraction, relapse of orthodontic treatment, and controlling the rotational axis of the teeth to remove crowding [8].
Ericsson et al. [9] noted that teeth movement without preorthodontic periodontal treatment could induce infrabony pockets since supra-gingival plaque goes under the gingiva along the movement. Wennström et al. [10] asserted that infrabony pockets would do no harm to clinical attachment if there was proper plaque control. Lindhe et al. [11] reported that orthodontic treatment after periodontal treatment can move teeth without attachment loss although it does not affect the clinical level itself in a positive way. Corrente et al. [12] wrote that an extruded tooth with an infrabony pocket showed decreased probing depth, clinical attachment gain, and bone filling radiographically after periodontal and orthodontic treatment. This study evaluates the effectiveness of periodontal treatment and a clear aligner for maxillary anterior PTM clinically and radiographically, based on the previous research mentioned above.
CASE DESCRIPTION
Subject
Three patients with chronic periodontitis and PTM who visited the Periodontal Department of the Chosun University Dental Hospital from May 2009 to July 2009 were sampled. Chronic periodontitis in the study is limited to cases accompanied by an infrabony pocket, tooth mobility ≤ 1°, and a sufficient amount of attached gingiva. Subjects for orthodontic treatment are defined as patients who have less than 4 mm PTM in the maxillary anterior area.
Clinical and radiographic examination
Clinical examination
The following clinical examinations were performed for the 3 patients pre- and post-periodontal and orthodontic treatment with a clear aligner.
Radiographic examination
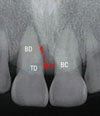
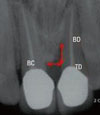
Subjects were checked to see if they had any infrabony pockets before periodontal treatment through panoramic and standard views. For the patients with an infrabony pocket, the vertical and horizontal size of the pocket was measured with the Infinitt π-ViewSTAR calipers at the Chosun University Dental Hospital Radiology System, as seen in Fig. 1. This method had been introduced by Corrente et al. previously (Fig. 1).
Treatment with clear aligner
After periodontal treatment, the clear aligner was applied. It was made on a patient's model cast, in which teeth were aligned after space analysis so that the patient's teeth would not be moved more than 1 mm by the appliance. Thermoplastic clear hard type (polyethylene) polymer was used with thicknesses of 0.5 mm and 0.75 mm. For the first week, a 0.5-mm-thick appliance was used, followed by a 0.75-mm-thick one for the subsequent two weeks. Patients were recalled every three weeks for new appliances. They were instructed to keep the appliance on all day long, with the exception of meal times.
Case reports
Case I
A 50-year-old male patient visited our department on July 14, 2009 with the chief complaint of anterior teeth sloping down and open. As mentioned above, clinical and radiographic examinations were performed (Tables 1 and 2, Fig. 2). He was diagnosed with chronic periodontitis localized in the maxillary anterior teeth area and pathologic tooth migration. The treatment plan was periodontal therapy to eliminate causes, tooth movement of 11, and prosthodontic treatment.
Figs. 3 and 4 show clinical photographs of the front side and the occlusal plane after periodontal treatment. As mentioned above, teeth were fixed at the location to where the teeth would shift with wax on the cast after space analysis (Figs. 5 and 6), and the clear aligner was fabricated (Fig. 7).
Figs. 8 and 9 show clinical photographs of the front side and the occlusal plane after 3 weeks. After space analysis, the teeth were fixed at the location where the teeth will be shifted to with wax again and the clear aligner was fabricated (Figs. 10 and 11).
Figs. 12 and 13 show photographs of the front side and occlusal plane after 6 weeks. Since the patient was satisfied with the results, use of a retention appliance was planned instead of prosthodontic treatment. After taking radiographs (Fig. 14), the retention appliance was applied (Fig. 15).
As a result, the probing pocket depth (PPD) and gingival recession (GR) decreased about 1 mm, and clinical attachment level (CAL) decreased about 2 mm when compared to the first visit. Also, mobility decreased slightly (Table 3).
In the radiographs, vertical and horizontal dimensions were measured (Table 4). Radiographically, the size of the infrabony defects decreased 0.8 mm vertically and 0.4 mm horizontally. However, actual bone filling in the lesions could not be determined based on the radiographic view alone.
Case II
A 34-year-old male patient visited our department on May 25, 2009, with chief complaints of anterior teeth separating and discomfort in the gums. As described above, clinical and radiographic examinations were performed (Tables 5 and 6, Fig. 16). He was diagnosed with an endo-perio lesion due to loss of tooth vitality and the pathologic tooth migration of 21. The treatment plan was periodontal therapy to eliminate causes, tooth movement of 11 and 21, and prosthodontic treatment.
Figs. 17 and 18 are clinical photographs of the front side and the occlusal plane after the periodontal treatment. As in case I, clinical photographs at the front side and occlusal plane views were taken after fabricating clear aligner on the cast and applying the device (Figs. 19 and 20). Figs. 21 and 22 are clinical photographs of the front side and occlusal plane views after 3 weeks of using the new appliance. A new appliance was applied again after 6 weeks (Figs. 23 and 24). Prosthodontic treatment was performed as planned (Figs. 25 and 26). After completing prosthodontic treatment, radiographs were taken for radiographic evaluation (Fig. 27).
To measure the results of the treatment, PPD, CAL, GR, and mobility were measured after treatment. GR and CAL decreased about 1 mm compared to the first visit, and mobility decreased slightly (Table 7).
In radiographs, the vertical and horizontal dimensions were measured after treatment (Table 8). Radiographically, the size of infrabony defects decreased 2.1 mm vertically and 0.7 mm horizontally. However, as in case I, actual bone filling in the lesions could not be determined based on the radiographic view alone.
Case III
The third patient was a 54-year-old male who visited our department June 11, 2009, with the chief complaint of anterior teeth sloping. Though clinical examination was performed as mentioned above (Table 9), no radiological examination was done due to the absence of the appearance of an infrabony defect (Fig. 28). He was diagnosed with chronic periodontitis localized on the 13-23 area and pathologic tooth migration. The treatment plan consisted of endodontic treatment, followed by periodontal therapy and tooth movement of 11 and 21, and prosthodontic treatment.
After periodontal treatment was performed (Figs. 29 and 30), an appliance was inserted (Figs. 31 and 32). Clinical photographs of the front side and occlusal plane were taken 6 weeks after appliance insertion (Figs. 33 and 34). Though prosthodontic treatment was recommended to the patient, the retention appliance was used. That's because the patient wanted to finish in the current state (Fig. 35). GR and CAL decreased about 1 mm compared to the first visit and there was no change in mobility (Table 10).
DISCUSSION
Many previous studies have been conducted on the combination of periodontal and orthodontic treatments for PTM in the maxillary anterior area. According to Melsen et al. [13] in 1989, the combination of treatments could induce the generation of new attachment tissue and clinical attachment gain if patients can maintain reasonable oral hygiene. In 2002, Re et al. [14] reported that periodontal patients with an infrabony pocket could decrease their bony lesions through orthodontic tooth movement. Corrente et al. [12] wrote in their 2003 article that rearrangement of extruded teeth with infrabony defects provided a significant decrease in probing depth, clinical attachment gain, and bone filling, which was identified in radiographic views. Previous research has already confirmed a decrease of PPD and clinical attachment gain. Decreases in the horizontal and vertical size of infrabony defects were also shown on radiographies, though actual bone filling has not been confirmed.
Retention should also be considered after the orthodontic treatment of periodontal patients. The final location of the teeth is determined by a balance of forces among the lips, cheeks, tongue, and periodontal ligament [15]. Periodontal patients whose periodontal tissue has been destroyed by strong soft tissue forces, therefore permanently disrupting the balance of forces, may therefore need permanent retention. The best retainer for those patients is flexible spiral wire [16]. In 1982, Nyman et al. [17] reported that splinting with a retainer had a positive effect on the attachment of connective tissue and bone regeneration.
In summary, to treat cases of PTM in the maxillary anterior area using a clear aligner, the first step is to determine the pathologic causes. If the condition stems from periodontal problems, general periodontal therapy should be performed. If the movement happens spontaneously, which is uncommon, the periodontal treatment has to be wrapped, and minimum tooth migration is done using a clear aligner. Permanent retention should follow.
A clear aligner is effective on partial movement of the teeth and it is reasonable, therefore, to expect decreases in probing pocket depth, gingival recession, clinical attachment gain, mobility, and esthetic recovery as a result of its use.









































 XML Download
XML Download