

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Surface modifications of titanium implants using various modalities aim to improve the initial healing and promote faster healing times [1]. With this surface modification, immediate or early loading has become a predictable treatment protocol [2]. Sand-blasted, large-grit, acid-etched (SLA) surfacing is one of these surface modifications. SLA surfacing has been shown to improve the clinical performance of implants [3,4]. Further modification of the SLA surface has been tested in an attempt to enhance implant stability [5,6].
Calcium phosphate (CaP) has bioactive and osteoconductive properties. It has been recognized that coating the surface of titanium implants with CaP can help to achieve rapid fixation and spontaneous binding to the neighboring bone [7,8]. Biological apatite, which can improve bone healing, is deposited on the surface of CaP-coated implants after implantation by the release of calcium and phosphate ions from the implant surface into the peri-implant region [8,9]. An ion-beam-assisted deposition (IBAD) method has recently been shown to improve the bond strength of the CaP coating layer [10,11].
Growth-factor-induced proliferation, differentiation, and migration have been shown to require the adhesion of cells to the extracellular matrix (ECM). Fibronectin, which is a major ECM component, is used as a substrate for cell attachment [12]. The first biological reaction at the interface between the biomaterial and tissue after implantation is the adsorption of body fluid proteins onto its surface, and subsequent biological responses at the interface are controlled by these adsorbed proteins [13,14]. The selective adsorption of beneficial molecules has been attempted by modifying the implant surfaces. It has beendemonstrated that coating the surface with cell-adhesive proteins, such as fibronectin, collagen, and/or laminin, improved initial cell attachment, cell spreading, and cell activity [15-18].
It has recently been recognized that biomimetic coating methods can improve the biological performance of implants. It has been reported that bone-like apatite was formed through coating, which involved soaking biomaterials in a simulated body fluid with ion concentrations similar to those found in human blood plasma. Biologically active molecules can be deposited with inorganic components and incorporated into the crystal lattice [19]. Biomimetic coating with fibronectin has been tested in previous studies [20-23]. It is believed that application of fibronectin to the implant surface can enhance the osseointegration of dental implants to the bone [20-23]. Fibronectin is one of the cell-adhesive proteins that can improve cell activity, initial cell attachment, and cell spreading, and it is actively involved in cytoskeletal reorganization and bone tissue formation, in part by regulating the survival of osteoblasts [24]. Fibronectin belongs to a group of high molecular weight glycoproteins that exist on cell surfaces. It is found in connective tissues, basement membranes, and extracellular fluids, and is known to play a role in cell-to-cell and cell-to-substrate adhesion [25], as well as an important role in osseointegration due to its capacity to make osteoblasts attach to ECM components. Furthermore, fibronectin has calcium-sensitive heparin-binding sites that should interfere with the biomineralization of titanium implants. Fibronectin adsorption onto solid substrates has already been evaluated in previous studies [26,27], though the interactions between this protein and biomaterial surfaces are not fully understood. Fibronectin is also known to enhance gingival fibroblast attachment, which has beneficial effects on healing after implant surgery and during the maintenance phase by forming attachments between connective tissue and the epithelium, which can prevent inflammatory breakdown around the implant. In contrast to natural teeth, cementum - into which gingival fibers can insert - does not exist around dental implants. Apical migration of the long junctional epithelium, which is the result of poor attachment between the subepithelial connective tissues and the epithelium around the implant, leads to the formation of peri-implant pockets. Inflammatory breakdown is caused by bacterial invasion through the peri-implant pocket [28,29]. The formation of a pocket around an implant can extend directly to the underlying bone in the absence of a transgingival seal between the gingival tissue and the implant. If this inflammatory breakdown extends to the underlying bone, the condition is defined as peri-implantitis, and can lead to implant failure [28].
The purpose of this study was to determine the effect of coating the implant surface with fibronectin on osseointegration.
MATERIALS AND METHODS
Animals
Four male, 18- to 24-month-old mongrel dogs weighing about 30 kg each were chosen. The dogs had intact dentition without any inflammation in the periodontium. The management, preparation, and surgical protocols used for the animals followed the standard protocols approved by the Animal Care and Use Committee of the Yonsei Medical Center, Seoul, Korea.
Sample preparation
SLA-surface-modified titanium implants (3.4 mm in diameter and 8.0 mm in length; Implantium, Dentium, Seoul, Korea) were used as substrates. The control condition was implantation of SLA-modified implants without fibronectin or CaP, while the experimental condition was implantation of SLA-modified implants that had been coated with a thin film of CaP, followed by fibronectin.
To prepare the Dulbecco's phosphate-buffered saline (DPBS) solution containing DPBS fibronectin (DPBSF), DPBS (calcium/magnesium free, Gibco BRL, San Diego, CA, USA) and reagent-grade CaCl2 (100 mg/L) were dissolved in distilled water. Details of the procedures for incorporating fibronectin into surfaces and deposition employed in this study have been described elsewhere [20]. Each SLA-surfaced implant coated with a thin film of CaP was immersed in 2.0 mL of DPBSF solution at 37℃ for 24 hours. The fibronectin-incorporated implants were then rinsed twice with distilled water and then air dried at ambient temperature. All of the solutions used were sterilized before use by filtration through a membrane with a pore size of 0.20 µm.
Study design
There were two groups separated by the surface condition of the implant (i.e., SLA- or fibronectin/CaP/SLA-surfaced). Healing was observed after 4 and 8 weeks. SLA-surfaced implants (n=8) were considered the control condition, and fibronectin/CaP-coated SLA-surfaced implants (n=8) as the experimental condition.
Surgical protocol
Mandibular premolars were extracted under general anesthesia and sterile conditions. Atropine was injected subcutaneously at 0.05 mg/kg, and 2 mg/kg xylazine (Rompun, Bayer Korea Ltd, Seoul, Korea) and 10 mg/kg ketamine hydrochloride (Ketalar, Yuhan, Seoul, Korea) were administered intravenously. The dogs were laid on a heating pad during surgery. An endotracheal tube was used for intubation, and anesthesia was maintained using 2% enflurane. The dogs were monitored with an electrocardiogram. After a 2-month healing period, 16 implants (8 SLA and 8 fibronectin-coated SLA) were placed into the edentulous mandibles as described below.
The animals were anesthetized as described above. A crestal incision was made and a full mucoperiosteal flap was raised. Two implant sites were identified on each side of the mandibles, and surgical preparation was performed according to the manufacturer's instructions using pilot and twist drills. Postoperative care was similar to that for tooth extraction. The sutures were removed after 7 to 10 days, and the dogs were fed a soft diet for 2 weeks. The dogs were sacrificed with an anesthesia overdose after either 4 or 8 weeks of healing.
Clinical and histologic analysis
Block sections including the segments with implants were preserved. They were fixed in 10% neutral buffered formalin, dehydrated in ethanol, embedded in methacrylate, and sectioned in the mesiodistal plane. The central section from each specimen was reduced to a 35-µm thickness by microgrinding (Exakt, Norderstedt, Germany). The sections were stained with Goldner's trichrome. Histologic evaluation was performed under an optical microscope (Leica Microsystems Wetzlar GmbH, Wetzlar, Germany).
Histometric analysis
Computer-assisted histometric measurements were made with an automated image-analysis system (Image-Pro Plus, Media Cybernetics, Silver Spring, MD, USA). Bone density (BD) and bone-to-implant contact (BIC) were measured histomorphometrically in the buccolingual plane. The percentage of BD in areas among the five coronal threads was calculated.
RESULTS
Clinical and histologic analysis
All implants were clinically stable and non-mobile. The osseointegration of each implant was confirmed. Osteoblasts had actively deposited osteoid matrix on the implant surface. The newly formed bone in the interthread space was in close contact with the implant surface, without any gaps or dense fibrous connective tissue. No apical epithelial migration was found. No inflammatory cell infiltrate was present around the implants. A few areas of bone remodeling with osteoblasts and osteoid matrix were observed.
Four-week time point
Fibronectin coating SLA group
Implants were stable without any mobility. The bone tissue surrounding implants is shown in Fig. 1. A greater amount of osteoid matrix (arrow), which is the unmineralized organic portion of bone matrix, was observed than uncoated SLA group. Newly formed bone which affected BIC and BD was also found in the interthread space.
SLA Group
Implants were stable without any mobility. The bone tissue surrounding implants is shown in Fig. 2. Osteoid matrix was also observed. A thin lining of newly formed bone was observed on the implant surface. Marrow space (arrow) near the osteoid matrix was observed. The amount of newly formed bone in the interthread space was less than for the other group.
Eight-week time point
Fibronectin coating SLA group
Implants were stable without any mobility. The bone tissue surrounding implants is shown in Fig. 3. Osseointegration of each implant was confirmed. Anincreased amount of newly formed mineralized bone in the interthread space was observed when compared with the 4-week fibronectin coated SLA group.
SLA group
Implants were stable without any mobility. The bone tissue surrounding implants is shown in Fig. 4. Osseointegration of each implant was confirmed. The newly formed bone in the interthread space was in close contact with the implant surface without any gaps or dense fibrous connective tissue. No apical epithelial migration was found. No inflammatory cell infiltrate was present around the implants. Anincreased amount of newly formed mineralized bone in the interthread space was observed when compared with the 4-week SLA group.
Histometric analysis
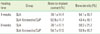
The mean values of BIC and BD were lower in the fibronectin/CaP-coated SLA group than in the SLA group after both 4 and 8 weeks of healing. The mean values of BIC and BD in both groups (fibronectin/CaP-coated SLA and SLA) were lower after 4 weeks of healing than at 8 weeks (Table 1). BIC and BD did not differ significantly between the groups.
DISCUSSION
The aim of the present study was to characterize the osseointegration of fibronectin/CaP-coated SLA-modified titanium dental implants. The BIC and BD of the coated implants were not greater than those of SLA implants without the fibronectin and CaP coating. Although the fibronectin/CaP coating of the SLA implant surface did not enhance osseointegration, it did not adversely affect healing in this canine study. There are several possible reasons for this, as discussed below.
Firstly, the canine model used in the present study was probably not sufficient to reveal any differences. The site preparation was performed according to the manufacturer's recommendations, without any defects. The SLA implants were coated with fibronectin after the surface had first been coated with a thin layer of CaP using the IBAD method, in which the original surface roughness is retained after coating. In a previous study using SLA implants coated with a thin layer of CaP to restore self-contained coronal defects in dogs, BIC and BD values that can be considered to reflect enhanced osseointegration were greater for SLA implants coated with a thin layer of CaP than for standard SLA implants [6]. In addition, a previous in vitro study with titanium discs coated with a thin layer of CaP followed by fibronectin found that the fibronectin that became incorporated into the apatite deposited on the surface of the titanium did not affect its biological activity in terms of promoting osteoblast attachment [20]. Therefore, in the present study, the fibronectin/CaP coating of SLA-modified titanium dental implants was expected to enhance osseointegration because 1) it had surface roughness, 2) a thin coating of CaP had already been shown to enhance osseointegration, and 3) a fibronectin coating has been shown to promote osteoblast attachment. However, enhanced osseointegration was not found in our canine model. Two osteogenetic phenomena have been proposed to occur around dental implants: distance and contact osteogenesis [30]. Distance osteogenesis takes place on the surface of the bone around the implant through appositional growth, while contact osteogenesis occurs directly on the surface of the implant. Contact osteogenesis was found to be enhanced more by a rough implant surface than by a smooth implant surface due to the increased surface area available for fibrin attachment and surface features to which fibrin could become attached. It is possible that fibronectin-coated SLA implants exhibit enhanced osseointegration in self-contained coronal defects in dogs because fibronectin has the ability to promote osteoblast attachment more via distance osteogenesis.
Secondly, it is not clear whether or not fibrin-coated fibronectin molecules preserve cell-adhesive activity after surgery. If the bond between the fibronectin coating and the substrate is not strong enough, the coating surface maybe exfoliated during surgery. Further study is necessary to examine changes in the cellular activity of cultured cells on the fibronectin-coated implant surface.
Thirdly, the healing period might not have been short enough to reveal any differences in healing due to coating the surfaces. Fibronectin affects healing in the early healing period. It may be that a difference would have been revealed if the healing had been evaluated after only 2 weeks. Future studies should examine the effects of applying a fibronectin-coated implant on early healing. In addition, the influence of fibronectin-coating SLA implants on long-term prognosis should be evaluated clinically. In particular, changes in soft-tissue healing, which can affect the long-term prognosis of implant therapy, should be evaluated. More rapid and enhanced soft-tissue healing around the implant may occur as a result of enhancement of epithelial cell attachment, spreading, and hemidesmosome assembly affected by the fibronectin coating applied to SLA implants. A canine model should be used to evaluate soft-tissue healing. In conclusion, the BD and BIC of fibronectin-coated implants were comparable to those of SLA-surfaced implants, which have been proven to be one of the most predictable implant types.




 XML Download
XML Download